 ISSN: 2822-0838 Online
ISSN: 2822-0838 Online

Differences in Ankle Dorsiflexion Deficit Performance between Male and Female Athletes with a History of Lateral Ankle Sprain: The Functional Pre-Participation Evaluation
Jatmiko, Damayanti Tinduh, Bambang Purwanto* and Andre Triadi DesnantyoPublished Date : April 3, 2023
DOI : https://doi.org/10.12982/NLSC.2023.017
Journal Issues : Number 2, April-June 2023
Abstract The objective of this study was to determine the effects of deficit of ankle dorsiflexion in athletes who sustained a chronic lateral ankle sprain to the hopping performance. A comparative study was designed to compare the deficit and non-deficit condition of ankle dorsiflexion as a result of the weight bearing lunges test to distance hopping ability with single leg hop, which was normalized with leg length. There were no statistically significant differences in hopping performance, deficit vs non-deficit ankle dorsiflexion within-group comparisons in males (P = 0.932) or females (P = 0.999). Between group comparisons showed that ankle dorsiflexion deficit among female resulted lower hopping performance compared to male with / without ankle dorsiflexion deficit (P = 0.041 and P = 0.039). Surprisingly, hopping performance among male with ankle dorsiflexion deficit was further than female without ankle dorsiflexion deficit (P = 0.044). Meanwhile, hopping performance between male versus female without ankle dorsiflexion deficit were not significant (P = 0.054). The deficit of ankle dorsiflexion had no influence on hopping performance in athlete with a history of LAS, both male and female. Sex influenced hopping performance in athletes with ankle dorsiflexion deficits, with female athletes performing worse than male. During recovery, there might be differences in biomechanical adaptation between ankle dorsiflexion deficit conditions in female athletes compared to male.
Keywords: Ankle-dorsiflexion deficit, Sex, Ankle sprain, Hopping distance, Adaptaion
Citation: Jatmiko, Tinduh, D., Purwanto, B., and Desnantyo, A.T. 2023. Differences in ankle dorsiflexion deficit performance between male and female athletes with a history of lateral ankle sprain: The functional pre-participation evaluation. Nat. Life Sci. Commun. 22(2): e2023017.
INTRODUCTION
Regular physical activity and exercise provide numerous health benefits, but they also carry risks, such as injury. In 2019, Herzog et al reported acute ankle sprains are the most common injury, representing approximately 15% of all injuries in sports activities. Lateral ankle sprain (LAS) was the most common type of ankle sprain and occurred most frequently during practice (Herzog et al., 2019) (Hodgkins and Wessling, 2021). Some athletes did not fully recover from LAS injuries, leading to an increased risk of developing Chronic Ankle Instability (CAI). It was reported that it accounted for approximately 32% of LAS incidents in athletes who developed CAI, with football having the highest prevalence of recurrent injuries and mechanical instability at 61%, followed by basketball at 60%. (Konradsen et al., 2002) (Koshino et al. 2020) (Attenborough et al., 2014). Individuals with a history of LAS and CAI had lower muscle strength, mechanical instability, proprioceptive loss, and decreased motor control due to kinematic compensation and maladaptation (Hertel and Corbett, 2019) (Wenning et al., 2020) (Xue et al. 2021) (Kim et al., 2019) (Nanbancha et al., 2019) Athletes also experienced several long-term consequences, such as a decrease in joint range of motion (ROM) dorsiflexion of the ankle. (Gribble et al., 2014) (Konradsen et al., 2002) (Hertel and Corbett, 2019)
Several research evaluated ankle dorsiflexion ability, both after a history of LAS injury or with CAI. As a result, there was a significant side-to-side absolute asymmetries in ankle dorsiflexion ROM (Miller, Fawcett, and Rushton 2020) (Hoch et al., 2012) (Kosik et al., 2019). The prevalence experienced by 38% - 67% of athletes following unilateral severe LAS injury (Clark and Campbell, 2021). The presence of talocrural joint arthrokinematic disturbances was one that influencing ankle dorsiflexion deficit. Others were triceps surae muscle flexibility disorders, neuromuscular control disorders, and post-injury ankle joint adaptation (Hertel, 2002) (Valderrabano et al., 2006) (Wikstrom and Hubbard, 2010) (Terada et al., 2014) (Kim et al., 2019). The maximum ROM of the ankle joint, used as a parameter in the clinical development of the rehabilitation program and the evaluation of the exercise intervention. The development of ankle dorsiflexion ROM was one of specific evaluation. (Collins, Teys, and Vicenzino, 2004).
After a LAS injury, ankle dorsiflexion ROM recovery was occurred over time, depended on the severity of the injury and the various clinical responses (Wisthoff et al., 2021) Some patients with a history of LAS or CAI, never regained their maximum ankle dorsiflexion ability (Wright et al., 2013). Athletes require maximum ankle dorsiflexion ability to support their performance in sports. Studies among normal athletes revealed that maximum ankle dorsiflexion contributed to dynamic balance, counter-movement jump performance, and energy efficiency when landing (Hoch, Staton, and McKeon, 2011) (Dowse et al., 2021) (Godinho et al., 2019).
Patients with a history of LAS or CAI reported ankle dorsiflexion deficits, which were associated with the possibility of ankle re-injury (Clark and Campbell, 2021), impaired dynamic balance (Hernández-Guillén et al., 2022), alterations in the lower limb kinematics (Aquino et al., 2022), and associated with dynamic knee valgus (Lima et al., 2018). Females were worse in dynamic knee valgus than males due to ankle dorsiflexion deficit (Arundale et al., 2020). However, it is was still unknown whether ankle dorsiflexion deficits influence hop distance. We hypothesized that ankle dorsiflexion deficits influence on hopping performance among individual with history of LAS. Among individual with ankle dorsiflexion deficit, hopping performance was lower in female compared to male.
MATERIALS AND METHODS
Materials
Data were collected during the East Java athletes' mandatory preparticipation physical evaluation, which performed by the Sport Clinic team of DR Soetomo Surabaya Hospital in both October 2017 and March 2020. The entire subject of the study performed a series of preseason competition functional tests, with ankle dorsiflexion ROM measured bilaterally using the Weight Bearing Lunges Test (WBLT) to ensure subjects met the inclusion criteria. Weight Bearing Lunges Test measurements produce relevant results and have a high correlation with laboratory examinations for assessing the functional ROM of the ankle dorsiflexion. The maximum distance of the lunge measured with the measuring tape and the inclinometer is a valid assessment, and it was chosen because it is less expensive, more reliable, and faster than other methods. This closed chain assessment of ankle dorsiflexion ROM was more externally generalizable measure of ankle mobility than open chain or non weight bearing methods (Hall and Docherty, 2017)(Konor, Morton, and Grindstaff, 2012).
Functional tests with hopping types were used to evaluate neuromuscular performance in a wide range of sports, including football (Read et al., 2019). The ability of hopping distances in single-leg hop and standing long jump tests in athletes with a history of injury could be used to identify the risk of re-injury in athletes during the competition season (Patterson et al., 2021). A shorter one-foot hop distance could indicate a higher risk of lower extremity injury (Collings et al., 2021). There were no significant differences in performance measures, when the injured limb was the dominant limb or when the injured limb was the non-dominant limb (Bansbach et al., 2017).
This study compared the hopping distance of a single leg hop for distance (SLHD) measurement, in the conditions of ankle dorsiflexion deficit and non-deficit at the side of injury as a result of the WBLT, in male and female athletes with a history of LAS. Prior to the group comparison, the hop distance from the selected subject was normalized by dividing it by their leg length (LL), which was measured from the anterior superior iliac spine to the medial malleolus (Munro and Herrington, 2011). This study was approved by the Research Ethics Committee at the Dr. Soetomo Hospital Ethics Committee, Surabaya, Indonesia, which states that this study complies with The Office for Human Research Protection under the requirements of the U.S. Department of Health and Human Services Regulation 45 CFR part 46 for exempt review. Approval number 0884/LOE/301.4.2/IV/2022, date of issue April 21, 2022
Subjects
A total sampling of all subjects who met the criteria was used, with the recognition that 38 data subjects were utilized to identify. Means and standard deviations were calculated as descriptive data for the participants' demographics, as shown in table 1. Thirty eight athlete data, men (n = 16) and women (n = 22) meet the criteria. In this study, the gender composition of athletes between groups that experienced deficits and non-deficits was consistent with Miller et al. finding's. As injured female athletes' WBLT ability is more limited, the population is larger than that of men, however the difference is not statistically significant (Miller, Fawcett, and Rushton, 2020).
Inclusion criteria were; (1) Data collected from ≥ 17-year-old athletes, who compete in weight-bearing type of sports such as; fencing, wrestling, wushu, hockey, athletics, gymnastics, basketball, water-skiing, handball, jump diving, kempo, and sepak takraw (2) Athletes reported at least one chronic LAS history on the questionnaire form, ≥ 6 months prior to the examination (3) The results of an ultrasonography test revealed a chronic sprain and/or a partial tear of the anterior talofibular ligaments (4) The screening results confirmed, that the athlete had a chronic ankle injury and/or a potential ankle injury (5) The result of WBLT on the injured side, either in deficit or non-deficit ankle dorsiflexion as measured by SLHD. Exclusion criteria were; (1) According to injury history, athletes have musculoskeletal injuries in other areas of the lower extremities, are experiencing low back pain, or have been diagnosed with concussion within 6 months of the examination. (2) Have been diagnosed with impaired balance, vestibular, neurological. (3) Have a history of fractures and/or a history of surgery on the lower extremities (Kosik et al., 2019).
Procedures
Data on health conditions and complaints were collected from all athletes who took part in the screening. The data from the questionnaire form was used to obtain the history of LAS injury, and all screening participants answered questions prior to the examination. The questionnaire stated that participation in the screening was voluntary, and that the results or data would be made anonymously to protect participants' privacy. Data from participants who met the inclusion criteria were analyzed, and the results were used to group measuring and control subjects. The Sport Clinic team performed the tests in accordance with the protocols. The WBLT data were collected by one of three physiotherapists with > 8 years clinical experience in sports medicine.
Weight bearing lunges test measurement using the toe to wall method, with the participant's bare foot facing the wall at the start (figure 1a). The measured foot correctly steps on a horizontal line marked on the floor with a marker placed in the center of the heel and thumb. Two measuring tapes were correctly aligned on the floor to the right and left of the line mark. Knees perpendicular to the wall, with vertical marking lines perpendicular to the horizontal line on the floor for easy supervision. Participants attached both palms to the wall to keep their balance and body upright during the test. Untested legs were placed on the floor, behind the measured feet, at a comfortable distance and with the heels raised. While maintaining that position, participants were instructed to perform a lunge in which the knees and ankles were bent until the center of the knees were attached or contacted to the vertical marking line of the wall while keeping the heels and toes aligned on the horizontal line on the floor. After completing the experiment, in which there was no change in the position of the heels against the floor, participants were instructed to move the soles of their feet away by about 5 cm. When the heel was lifted from the floor, the sole of the foot advanced forward until the heel makes contact with the floor. With the correction of the marker, the contact of the knee with the wall and the contact of the heel with the floor are visually monitored. A perpendicular projection of the fingertips with a measuring tape was the result of the measurement (figure 1b) (Hoch et al., 2012) (Konor, Morton, and Grindstaff, 2012) (Chisholm et al., 2012) (Langarika-Rocafort et al., 2017).

Figure 1. WBLT screening procedure. (a) Position at the time of measurement. (b) Projection of the fingertips to measuring tape.
Data from ankle dorsiflexion deficits greater than 1.5 cm above baseline (> 1.5 cm) were included in the measuring group, Those who were less than 1.5 cm below baseline (≤ 1.5 cm) were included in the control group. (Hoch and McKeon 2011). Participants with a history of bilateral LAS, as well as lower limbs with ankle dorsiflexion asymmetry greater than baseline (> 1.5 cm), were included in the deficits group. Data were collected from all subjects who performed the SLHD on the lower limbs in each group. Subjects were shown a demonstration and given standardized instructions before being measured for SLHD. Data were taken with in the participant relaxed stand position on singular foot of his or her fingertips correctly on the starting line mark Participants performed one jump, land without losing balance, and hold the final landing position for at least two seconds. To avoid performance bias due to the influence of the injured side, side, the test started firstly with normal limb. There were no obstacles to free arm movements during the test. The hopping distance is measured from the tip of the toe during takeoff to the tip of the toe during landing on the same foot. For each test, one attempted hop was followed by two measured hops (Reid et al., 2007) (Witchalls et al., 2013). The hop was considered unsuccessful if there is a loss of balance at the end of the hop, additional jumping motion when landing, or the lower extremities of the contralateral or upper extremities touch the floor when landing (Munro and Herrington, 2011).
Statistical analyses
The Shapiro-Wilk test resulted the data distribution was significantly different to a normal data distribution pattern so that non-parametric test of Kruskal-Wallis was used to compare data between four groups and followed by Games-Howell post Hoc test. Statistical significance was set to P < 0.05. All statistical procedures were performed using SPSS Statistics (IBM Corp. IBM SPSS Statistics for Windows, Version 16. Armonk, NY, USA).
RESULTS
The male deficit consists of 7 subjects, with 1 subject experiencing bilateral LAS, the female deficit consists of 11 subjects, with 3 subjects experiencing bilateral LAS, the male non-deficit consists of 9 subjects with unilateral LAS, and the female non-deficit consists of 11 subjects with unilateral LAS. A chi-square analysis of the four groups reveals no statistically significant differences in age, mass, height, body mass index, and leg length. The subject characteristics were seen at table 1.
Ankle dorsiflexion deficit did not influence on single leg hop for distance among male and female subjects. Single leg hop for distance did not difference between male deficit group's compare to male non deficit group’s (P = 0.932). Similar result was found among female (P = 0.999). The history of LAS resulted lower single leg hop for distance among female subject compared to male subject. Ankle dorsiflexion deficit among female with LAS history resulted lower single leg hop for distance compared to male with / without ankle dorsiflexion deficit (P = 0.041 and P = 0.039). Surprisingly, single leg hop for distance among male with ankle dorsiflexion deficit was further than female without ankle dorsiflexion deficit (P = 0.044). Meanwhile, comparison results between male and female without ankle dorsiflexion deficit were not significant (P = 0.054). Comparison of single leg hop for distance between ankle dorsiflexion deficit vs non deficit with history of LAS was seen at figure 2.
Table 1. Subject characteristics between groups, represented in mean ± SD.
|
|
Male deficit (n = 7) |
Female deficit (n = 11) |
Male non deficit (n = 9) |
Female non deficit (n = 11) |
Significance between groups (P) |
|
Age (years) |
24.6 ± 5.2 |
20.5 ± 2.0 |
25.5 ± 6.6 |
23.4 ± 4.1 |
0.533 |
|
Mass (kg) |
66.6 ± 7.4 |
56.8 ± 5.7 |
63.8 ± 7.2 |
57.9 ± 10.5 |
0.403 |
|
Height (cm) |
170 ± 6.9 |
160 ± 6.5 |
169.3 ± 3.7 |
162 ± 6.4 |
0.579 |
|
BMI |
23 ± 1.2 |
22.2 ± 1.8 |
22.2 ± 1.8 |
21.9 ± 3.1 |
0.463 |
|
Leg length (cm) |
91.1 ± 5.2 |
91.5 ± 7 |
92 ± 4.7 |
88.9 ± 6.4 |
0.341 |
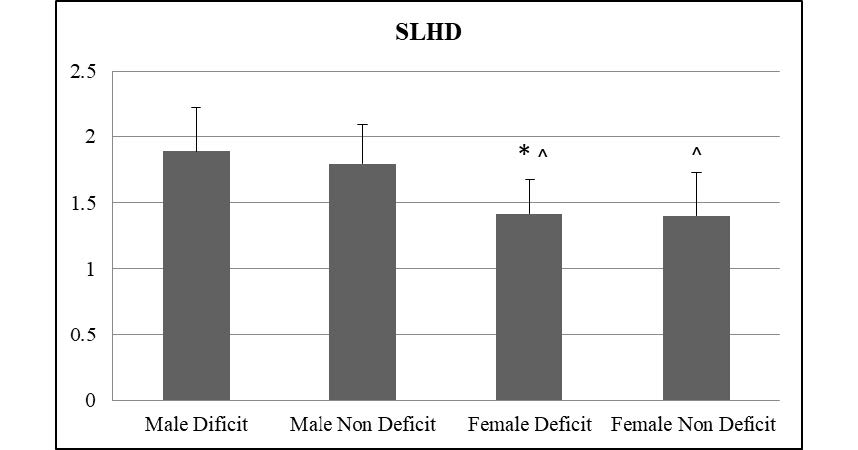
Figure 2. Comparison of single leg hop for distance between ankle dorsiflexion deficit vs non deficit with history of LAS among male and female subject. Analized with Kruscal Wallis, Games-Howell post hoc test *significant differences against the male non-deficit group (P <0.05); ^significant to the male deficit group (P <0.05); SLHD = Single Leg Hop for Distance
DISCUSSION
Similar sexes comparison groups
A Games-howell post hoc comparison of hopping distance measured with SLHD at injury limbs of each gender revealed that male athletes with ankle dorsiflexion deficits had no significant difference in hopping distance (P > 0.05) compared to male athletes without deficits of ankle dorsiflexion. Similarly, female athletes with ankle dorsiflexion deficits did not differ significantly compared to female athletes without ankle dorsiflexion deficits (P > 0.05). Our results contradicted with our hypothesis as there is no one difference was noted. The mean of SLHD in male deficit hopping distance results is shown further (figure 2). However, the post-hoc comparison with male non-deficit was not significant. The mean of SLHD was comparable in both deficit and non-deficit female athletes (figure 2). The post hoc comparison of female athletes with and without ankle dorsiflexion deficits was not significant.
Previous research in female athletes found that, ankle flexibility is not associated with agility or running performance (Richardson and DeBeliso, 2020). Similarly, in men, research from the trained military group found no significant difference in performance between limbs with a history of LAS injury and those with normal control (Bansbach et al., 2017). In adult male athletes also reported, that functional performance comparisons between the CAI groups and normal controls revealed no significant differences (Lu et al., 2022) (Navarro-Santana et al., 2019). Previous study by Navarro-Santana et al found, no difference in the explosive performance ability of the lower limbs when vertical jumping with CAI conditions, but there was an effect on the performance of lower limb endurance when side hops on CAI (Ko, Rosen, and Brown, 2018).
Another study compared the muscle strength ratios of the injured and normal sides of football, volleyball, and basketball players, the results were not significant. The measurement of muscle strength ratio should take into account factors that affect muscle strength such as type of injury, severity of injury, and sport type (Vosburg et al., 2022). The ability to hop between the lower limbs varies with each active adult healthy individual, resulting in asymmetry between normal limbs and CAI, with an average symmetry index above 90% (Madsen et al., 2020). In 2021, Simon et al reported the symmetry index between the limbs when performing SLHD is not significant between pre- and post-injury conditions, when the athlete has returned to sport activity. However, there is compensation on the side of the injury that affects the lower limb symmetry profile. (Simon, Yom, and Grooms, 2021). A chronic condition in which athletes have returned to sports following a LAS injury with a specific training pattern, allowing adaptation to occur. The condition resulted in an ankle dorsiflexion deficit, because various factors after LAS injury, did not affect hop distance. The subject had already discovered a solution to its deficiencies. Athletes with a history of chronic LAS who are already returning to sport with ankle dorsiflexion deficit conditions can hop just as well as the same gender's non deficit ankle dorsiflexion group. Future investigation might examine the biomechanics profile of athletes with dorsiflexion limitations after LAS
Different sexes comparison groups
Female athletes' hopping distances measured with SLHD differed from male athletes'. Figure 2 showed that post hoc comparison of SLHD between female athletes with ankle dorsiflexion deficits were significantly shorter than male athletes with ankle dorsiflexion deficits (P < 0.05). Female athletes with ankle dorsiflexion deficits had significantly shorter SLHD than male athletes without ankle dorsiflexion deficits (P < 0.05). It is supporting our prior hypothesis. Surprisingly, female athletes without ankle dorsiflexion deficit had shorter SLHD than male athletes with dorsiflexion deficit (P < 0.05). However, the comparison results between female and male athletes in the same condition without ankle dorsiflexion deficit were not significant (P > 0.05). It contradicts the SLHD comparison between female and male athletes with ankle dorsiflexion deficits. Several studies had compared sexes, even in the history of LAS or with CAI, especially in terms of biomechanical differences. Female athletes with ankle dorsiflexion deficits had lower functional test ability than male athletes (Chimera, Smith, and Warren, 2015) (Lu et al., 2022). In 2018, Onate et al reported the difference in SLHD test performance between sexes in normal high school athletes, that males tended to demonstrate greater single-legged–hop capabilities than females (Onate et al., 2018).
In contrast with ankle dorsiflexion deficit condition, the non-significant results of female athletes without ankle dorsiflexion deficits compared to male athletes give rise to the notion that female athletes are more likely to be affected by ankle dorsiflexion deficits than male athletes. Male athletes with deficit ankle dorsiflexion develop coping mechanisms if ankle dorsiflexion without deficit is a normal condition of functional recovery after LAS. Female deficit cannot compensate for deficiencies as well as male deficit. Female athletes performed significantly worse on ankle dorsiflexion deficit, most likely due to changes in neuromuscular control and adaptation during post-LAS injury recovery. Under normal conditions, the deficit of ankle dorsiflexion in female athlete is associated with biomechanical changes in the lower extremities during jump - landing activities (Taylor et al., 2022). In 2019, Chen et al. reported that postural stability control patterns in healthy populations revealed gender differences (Chen et al., 2019). Female use ankle strategies to maintain body balance more than men, whereas CAI patients have proprioceptive deficits and kinesthesia of inversion motion and plantar ankle flexion (Olchowik et al., 2015) (Xue et al., 2021). This phenomenon is associated with a slower onset of peroneus longus and anterior tibial muscle activity in people with CAI compared to the control group during perturbation of posture balance, ventral and dorsal directions (Labanca et al., 2021). It was also reported that patients with CAI had lower leg pronation deviation during sprinting activities when compared to healthy subjects. As the running distance increases, the decline becomes more pronounced (Colapietro et al., 2020). These findings are likely to influence on gait in women with CAI, where there is a significant decrease in gait performance compared to non-CAI women and men with CAI. (Lee, Lee, and Ha, 2021)
Observations of jump-landing motion in normal female athletes revealed that the ability of ankle dorsiflexion was related to the level of knee and hip flexion and the absorbency of the hip and knee extensor muscles, as well as deviations in frontal field knee movements. Female athletes do not make full use of their ankle dorsiflexion ROM (Taylor et al., 2022). The findings of the previous observations are consistent with the findings of Labanca et al. who discovered that ankle stability in female CAI patients is related to hip abductor strength (Labanca et al., 2021). In addition, Lu et al. discovered a decrease in hip abductor muscle strength in female CAI patients, with results that were significantly lower than those of male CAI patients (Lu et al., 2022). Kline et al. found that in normal subjects, the strength of the proximal muscles of the hips, including external rotators, affects hop performance in addition to the strength of the knee extensor, so that females with a history of LAS require greater activation of the hip muscles when performing movements (Kline et al., 2018) (Lu et al., 2022). Another risk associated with adult female athletes' biomechanical compensation is a greater valgus angle of the knee during the initial contact phase and the maximum knee flexion phase during landing. Women's movement patterns that develop in the presence of an increased angle of abduction of the knee will contribute to a higher load on the knee joint. The condition increases the risk of lower extremity and post-menstrual knee injury (Sonesson et al., 2022).
The use of ankle strategies in females with a history of LAS injury is likely to change (Olchowik et al., 2015) (Colapietro et al., 2020) (Labanca et al., 2021) (Xue et al., 2021). According to the lower limbs kinetic chain concept, changes in the area of the ankle joint following chronic LAS are likely to trigger kinematic compensation and changes in motion control, including activation of the proximal area of the lower limb (Terada, Pietrosimone, and Gribble 2013) (Kim et al., 2019) (Howe et al., 2021) (Labanca et al., 2021). This condition requires greater hip muscle strength, but female athletes with a history of LAS or CAI tend to have lower muscle strength, both abductors and external rotators than male athletes (Labanca et al., 2021) (Lu et al., 2022). Kinematic changes resulting from ankle dorsiflexion deficits are likely to occur in the CNS. Changes in corticomotor nerve excitability and inhibition in CAI patients indicate the presence of a cortical maladaptation process. (Kim et al., 2019) (Pietrosimone and Gribble, 2012) (Futatsubashi et al., 2013) (Nanbancha et al., 2019). In female, the condition is likely to cause non-optimal hop preparations due to a decrease in proximal muscle strength and kinematic changes, affecting the strength of the hopping prime mover muscles (Kline et al., 2018).
Thus, the current findings revealed that the hopping distance of female athletes with ankle dorsiflexion deficit is significantly lower than male. There may be differences in biomechanical adaptation between ankle dorsiflexion deficit conditions in female athletes compared to male athletes. As a result, it is essential to consider the gender differences and activity level when evaluating performance after LAS (Onate et al., 2018) (Lu et al., 2022). In the normal condition of athletes demonstrates that, gender has a significant influence on SLHD performance tests. Male athletes with a high level of activity have greater abilities than female athletes (Onate et al., 2018). Future research might examine the impact of ankle dorsiflexion limitations through female athletes following LAS or CAI
This study is not without limitation. The current study is based on the results of preseason competition multi-event screenings across multiple sports. The diversity of sports and training patterns within each group maybe influence hop outcomes. Future research should compare performance in ankle dorsiflexion deficits and non-deficits after LAS by grouping subjects with the same sport. The findings of this study could not differentiate between the types of kinematic adaptation and specific muscle recruitment in athletes with deficit and non-deficit ankle dorsiflexion, or between male and female with a history of LAS. Future research involving biomechanical analysis and muscle recruitment is required to assess the characteristic.
CONCLUSION
This study revealed that a deficit of ankle dorsiflexion had no influence on hopping performance in athlete with a history of chronic LAS, both male and female. Sex influenced hopping performance in athletes with ankle dorsiflexion deficits. Female athletes with a deficit in ankle dorsiflexion had lower hopping performance than male athletes. During the recovery process after LAS injury, there may be differences in biomechanical adaptation between ankle dorsiflexion deficit conditions in female athletes compared to male. Further, clinicians are expected to consider gender, activity level, and sport when determining the limitation performance following LAS injury.
ACKNOWLEDGMENTS
The authors thank the Dr. Soetomo General Academic Hospital for providing data.
AUTHOR CONTRIBUTIONS
Jatmiko conception, performance of work, performed the statistical analysis and data visualization, wrote the manuscript. Damayanti Tinduh conception, supervision, revision for important intellectual content. Bambang Purwanto conception, supervision, revision for important intellectual content, performed the statistical analysis and data visualization. Andre Triadi Desnantyo supervision, revision for important intellectual content. All authors have read and approved of the final manuscript.
CONFLICT OF INTEREST
The authors have no conflicts of interest to report.
REFERENCES
Aquino, M.R.C., Resende, R.A., Kirkwood, R.N., Souza, T.R., Fonseca, S.T., and Ocarino, J.M. 2022. Spatial-temporal parameters, pelvic and lower limb movements during gait in individuals with reduced passive ankle dorsiflexion. Gait and Posture 93 (December 2021): 32–38.
Arundale, Amelia J.H., Kvist, Joanna, Hägglund, Martin, and Fältström, Anne. 2020. Jump performance in male and female football players. Knee Surgery, Sports Traumatology, Arthroscopy. 28: 606–613.
Attenborough, A.S., Hiller, C.E., Smith, R.M., Stuelcken, M., Greene, A., and Sinclair, P.J. 2014. Chronic ankle instability in sporting populations. Sports Medicine. 44: 1545–1556.
Bansbach, H.M., Lovalekar, M.T., Abt, J.P., Rafferty, D., Yount, D., and Sell, T.C. 2017. Military personnel with self-reported ankle injuries do not demonstrate deficits in dynamic postural stability or landing kinematics. Clinical Biomechanics 47 (June 2016): 27–32.
Chen, Z., Han, J., Waddington, G., Adams, R., and Witchalls, J. 2019. Somatosensory perception sensitivity in voluntary postural sway movements: Age, gender and sway effect magnitudes. Experimental Gerontology. 122: 53–59.
Chimera, N.J., Smith, C.A., and Warren, M. 2015. Injury history, sex, and performance on the functional movement screen and y balance test. Journal of Athletic Training. 50: 475–485.
Chisholm, M.D., Birmingham, T.B., Brown, J., MacDermid, J., and Chesworth, B.M. 2012. Reliability and validity of a weight-bearing measure of ankle dorsiflexion range of motion. Physiotherapy Canada. 64: 347–355.
Clark, N.C. and Campbell, S.D. 2021. Preseason weight-bearing ankle dorsiflexion in male professional football players with and without a history of severe ankle injury: A Novel analysis in an english premier league club. Physical Therapy in Sport. 52: 21–29.
Colapietro, M., Fraser, J.J., Resch, J.E., and Hertel, J. 2020. Running mechanics during 1600 meter track runs in young adults with and without chronic ankle instability. Physical Therapy in Sport. 42: 16–25.
Collings, T.J., Bourne, M.N., Barrett, R.S., Moulin, W. du, Hickey, J.T., and Diamond, L.E. 2021. Risk factors for lower limb injury in female team field and court sports: A systematic review, meta-analysis, and best evidence synthesis. Sports Medicine. 51: 759–776.
Collins, N., Teys, P., and Vicenzino, B. 2004. The initial effects of a mulligan’s mobilization with movement technique on dorsiflexion and pain in subacute ankle sprains. Manual Therapy. 9: 77–82.
Dowse, R.A., Secomb, J.L., Bruton, M., and Nimphius, S. 2021. Ankle proprioception, range of motion and drop landing ability differentiates competitive and non-competitive surfers. Journal of Science and Medicine in Sport. 24: 609–613.
Elsevier B.V. Langarika-Rocafort, A., Emparanza, J.I., Aramendi, J.F., Castellano, J., and Calleja-González, J. 2017. Intra-rater reliability and agreement of various methods of measurement to assess dorsiflexion in the weight bearing dorsiflexion lunge test (WBLT) among female athletes. Physical Therapy in Sport. 23: 37–44.
Futatsubashi, G., Sasada, S., Tazoe, T., and Komiyama, T. 2013. Gain modulation of the middle latency cutaneous reflex in patients with chronic joint instability after ankle sprain. Clinical Neurophysiology. 124: 1406–1413.
Godinho, I., Pinheiro, B.N., Scipião Júnior, L.D.G., Lucas, G.C., Cavalcante, J.F., Monteiro, G.M., and Uchoa, P.A.G. 2019. Effect of reduced ankle mobility on jumping performance in young athletes. Motricidade. 15: 46–51.
Gribble, P.A., Delahunt, E., Bleakley, C.M., Caulfield, B., Docherty, C.L., Fong, D.T.P., Fourchet, F., Hertel, J., Hiller, C.E., Kaminski, T.W., et al. 2014. Selection criteria for patients with chronic ankle instability in controlled research: A position statement of the international ankle consortium. Journal of Athletic Training. 49: 121–127.
Hall, E.A. and Docherty, C.L. 2017. Validity of clinical outcome measures to evaluate ankle range of motion during the weight-bearing lunge test. Journal of Science and Medicine in Sport. 20: 618–621.
Hernández-Guillén, D., Roig-Casasús, S., Tolsada-Velasco, C., García-Gomáriz, C., and Blasco, J.M. 2022. Talus Mobilization-based manual therapy is effective for restoring range of motion and enhancing balance in older adults with limited ankle mobility: A randomized controlled trial. Gait and Posture. 93: 14–19.
Hertel, J. and Corbett, R.O. 2019. An Updated Model of chronic ankle instability. Journal of Athletic Training. 54: 572–588.
Hertel, J. 2002. Functional anatomy, pathomechanics, and pathophysiology of lateral ankle instability. Journal of Athletic Training. 37: 364–375.
Herzog, M.M., Kerr, Z.Y., Marshall, S.W., and Wikstrom, E.A. 2019. Epidemiology of ankle sprains and chronic ankle instability. Journal of Athletic Training. 54: 603–610.
Hoch, M.C. and McKeon, P.O. 2011. Normative range of weight-bearing lunge test performance asymmetry in healthy adults. Manual Therapy. 16: 516–519.
Hoch, M.C., Staton, G.S., and McKeon, P.O. 2011. Dorsiflexion range of motion significantly influences dynamic balance. Journal of Science and Medicine in Sport. 14: 90–92.
Hoch, M.C., Staton, G.S., Medina McKeon, J.M., Mattacola, C.G., and McKeon, P.O. 2012. Dorsiflexion and dynamic postural control deficits are present in those with chronic ankle instability. Journal of Science and Medicine in Sport. 15: 574–579.
Hodgkins, C.W. and Wessling, N.A. 2021. Epidemiology of sports-specific foot and ankle injuries. Foot and Ankle Clinics. 26: 173–185.
Howe, L., North, J.S., Waldron, M., and Bampouras, T.M. 2021. Restrictions in ankle dorsiflexion range of motion alter landing kinematics but not movement strategy when fatigued. Journal of Sport Rehabilitation. 30: 911–119.
Kim, H., Son, S.J., Seeley, M.K., and Hopkins, J.T. 2019. Altered movement strategies during jump landing/cutting in patients with chronic ankle instability. Scandinavian Journal of Medicine and Science in Sports. 29: 1130–1140.
Kline, P.W., Burnham, J., Yonz, M., Johnson, D., Ireland, M.L., and Noehren, B. 2018. Hip external rotation strength predicts hop performance after anterior cruciate ligament reconstruction. Knee Surgery, Sports Traumatology, Arthroscopy. 26: 1137–1144.
Ko, J., Rosen, A.B., and Brown, C.N. 2018. Functional performance deficits in adolescent athletes with a history of lateral ankle sprain(S). Physical Therapy in Sport. 33: 125–132.
Konor, M.M., Morton, S., and Grindstaff, T.L. 2012. Reliability of three measures of ankle dorsiflexion range of motion. International Journal of Sports Physical Therapy. 7: 279–288.
Konradsen, L., Bech, L., Ehrenbjerg, M., and Nickelsen, T. 2002. Seven years follow-up after ankle inversion trauma. Scandinavian Journal of Medicine and Science in Sports. 12: 129–135.
Koshino, Y., Samukawa, M., Murata, H., Osuka, S., Kasahara, S., Yamanaka, M., and Tohyama, H. 2020. Prevalence and characteristics of chronic ankle instability and copers identified by the criteria for research and clinical practice in collegiate athletes. Physical Therapy in Sport. 45: 23–29.
Kosik, K.B., Johnson, N.F., Terada, M., Thomas, A.C., Mattacola, C.G., and Gribble, P.A. 2019. Decreased dynamic balance and dorsiflexion range of motion in young and middle-aged adults with chronic ankle instability. Journal of Science and Medicine in Sport. 22: 976–980.
Labanca, L., Mosca, M., Ghislieri, M., Agostini, V., Knaflitz, M., and Benedetti, M.G. 2021. Muscle activations during functional tasks in individuals with chronic ankle instability: A Systematic review of electromyographical studies. Gait and Posture. 90:340-373.
Lee, I., Lee, S.Y., and Ha, S. 2021. “Alterations of lower extremity function, health-related quality of life, and spatiotemporal gait parameters among individuals with chronic ankle instability. Physical Therapy in Sport. 47: 46–52.
Lima, Y.L., Ferreira, V.M.L., Paula Lima, P.O. de, Bezerra, M.A., Oliveira, R.R. de, and Almeida, G.P.L. 2018. The association of ankle dorsiflexion and dynamic knee valgus: A systematic review and meta-analysis. Physical Therapy in Sport. 29: 61–69.
Lu, J., Wu, Z., Adams, R., Han, J., and Cai, B. 2022. Sex differences in the relationship of hip strength and functional performance to chronic ankle instability scores. Journal of Orthopaedic Surgery and Research. 17: 1–7.
Madsen, L.P., Booth, R.L., Volz, J.D., and Docherty, C.L. 2020. Using Normative data and unilateral hopping tests to reduce ambiguity in return-to-play decisions. Journal of Athletic Training. 55: 699–706.
Miller, H., Fawcett, L., and Rushton, A. 2020. Does gender and ankle injury history affect weightbearing dorsiflexion in elite artistic gymnasts? Physical Therapy in Sport. 42: 46–52.
Munro, A.G. and Herrington, L.C. 2011. Between-session reliability of four hop tests and the agility T-test. Journal of Strength and Conditioning Research. 25: 1470–1477.
Nanbancha, A., Tretriluxana, J., Limroongreungrat, W., and Sinsurin, K. 2019. Decreased supraspinal control and neuromuscular function controlling the ankle joint in athletes with chronic ankle instability. European Journal of Applied Physiology. 119: 2041–2052.
Navarro-Santana, M.J., Albert-Lucena, D., Gómez-Chiguano, G.F., Plaza-Manzano, G., Fernández-de-las-Peñas, C., Cleland, J., Pérez-Silvestre, Á., and Asín-Izquierdo, I. 2019. Pressure pain sensitivity over nerve trunk areas and physical performance in amateur male soccer players with and without chronic ankle instability. Physical Therapy in Sport. 40: 91–98.
Olchowik, G., Tomaszewski, M., Olejarz, P., Warchoł, J., Różańska-Boczula, M., and Maciejewski, R. 2015. The human balance system and gender. Acta of Bioengineering and Biomechanics. 17: 69–74.
Onate, J.A., Starkel, C., Clifton, D.R., Best, T.M., Borchers, J., Chaudhari, A., Dawn Comstock, R., Cortes, N., Grooms, D.r., et al. 2018. normative Functional Performance Values in high school athletes: The functional pre-participation evaluation project. Journal of Athletic Training. 53: 35–42.
Patterson, C.S., Dudley, R.I., Sorenson, E., and Brumitt, J. 2021. Preseason functional tests discriminate injury risk in female collegiate volleyball players. Physical Therapy in Sport. 51: 79–84.
Pietrosimone, B.G. and Gribble, P.A. 2012. Chronic ankle instability and corticomotor excitability of the fibularis longus muscle. Journal of Athletic Training. 47: 621–626.
Read, P.J., Oliver, J.L., Croix, M.B.A.D., Myer, G.D., And, and Lloyd, R.S. 2019. A review of field-based assessments of neuromuscular control and their utility in male youth soccer players. Journal of Strength and Conditioning Research. 33: 283–299.
Reid, A., Birmingham, T.B., Stratford, P.W., and Alcock, G.K. 2007. Hop Testing provides a reliable and valid outcome measure during rehabilitation after anterior cruciate ligament reconstruction. Physical Therapy. 87: 337–349.
Richardson, J. and DeBeliso, M. 2020. The relationship between ankle flexibility, agility, and sprint speed performance in collegiate female athletes. European Journal of Physical Education and Sport Science. 6: 97–112.
Simon, J.E., Yom, J., and Grooms, D.R. 2021. Symmetry does not indicate recovery: Single-leg hop before and after a lower extremity injury. International Journal of Sports Medicine. 42: 344–349.
Sonesson, S., Hägglund, M., Kvist, J., Torvaldsson, K., Lindblom, H., and Fältström, A. 2022. Neuromuscular control and hop performance in youth and adult male and female football players. Physical Therapy in Sport. 55: 189–195.
Taylor, J.B., Wright, E.S., Waxman, J.P., Schmitz, R.J., Groves, J.D., and Shultz, S.J. 2022. Ankle dorsiflexion affects hip and knee biomechanics during landing. Sports Health. 14: 328–335.
Terada, M., Harkey, M.S., Wells, A.M., Pietrosimone, B.G., and Gribble, P.A. 2014. The influence of ankle dorsiflexion and self-reported patient outcomes on dynamic postural control in participants with chronic ankle instability. Gait and Posture. 40: 193–197.
Terada, M., Pietrosimone, B.G., and Gribble, P.A. 2013. Therapeutic interventions for increasing ankle dorsiflexion after ankle sprain: A systematic review. Journal of Athletic Training. 48: 696–709.
Valderrabano, V., Hintermann, B., Horisberger, M., and Tak, S.F. 2006. Ligamentous posttraumatic ankle osteoarthritis. American Journal of Sports Medicine. 34: 612–620.
Vosburg, E., Hinkey, M., Meyers, R., Csonka, J., Salesi, K., Siesel, T., Fonseca, J., Zarzour, R., Sell, T., and Faherty, M. 2022. The association between lower extremity strength ratios and the history of injury in collegiate athletes. Physical Therapy in Sport. 55: 55–60.
Wenning, M., Gehring, D., Mauch, M., Schmal, H., Ritzmann, R., and Paul, J. 2020. Functional deficits in chronic mechanical ankle instability. Journal of Orthopaedic Surgery and Research. 15: 1–8.
Wikstrom, E.A. and Hubbard, T.J. 2010. Talar positional fault in persons with chronic ankle instability. Archives of Physical Medicine and Rehabilitation. 91: 1267–1271.
Wisthoff, B.A, Docherty, C.L., Glutting, J., Gustavsen, G., Royer, T.D, Swanik, C., and Kaminski, T.W. 2021. Identifying range-of-motion deficits and talocrural joint laxity after an acute lateral ankle sprain. Journal of Athletic Training. 56: 408-417.
Witchalls, J.B., Newman, P., Waddington, G., Adams, R., and Blanch, P. 2013. Functional performance deficits associated with ligamentous instability at the ankle. Journal of Science and Medicine in Sport. 16: 89–93.
Wright, C.J., Arnold, B.L., Ross, S.E., Ketchum, J., Ericksen, J., and Pidcoe, P. 2013. Clinical examination results in individuals with functional ankle instability and ankle-sprain copers. Journal of Athletic Training. 48: 581–589.
Xue, X., Ma, T., Li, Q., Song, Y., and Hua, Y. 2021. Chronic ankle instability is associated with proprioception deficits: A systematic review and meta-analysis. Journal of Sport and Health Science. 10: 182–191.
OPEN access freely available online
Chiang Mai University Journal of Natural Sciences [ISSN 16851994]
Chiang Mai University, Thailand.
https://cmuj.cmu.ac.th
Jatmiko 1, Damayanti Tinduh 1, 2, Bambang Purwanto1, * and Andre Triadi Desnantyo1, 2
1 Sport Health Science, Post Graduate Program, Faculty of Medicine, Universitas Airlangga, Surabaya 60131, Indonesia.
2 Dr. Soetomo General Academic Hospital, Surabaya 60286, Indonesia
Corresponding author: Bambang Purwanto, E-mail: bpaifo@gmail.com
Total Article Views
Editor: Areewan Klunklin,
Chiang Mai University, Thailand
Article history:
Received: August 4, 2022;
Revised: November 22, 2022;
Accepted: November 28, 2022;
Published online: December 6, 2022