 ISSN: 2822-0838 Online
ISSN: 2822-0838 Online

Assessment of the Antihyperlipidemic Effect of Garlic Vs Pitavastatin in Patients with Moderate Hyperlipidemia: A Metanalysis of Randomized Controlled Trials
Muhammad Waqas Saeed, Syed Wasif Gillani*, Rana Kamran Mahmood, and Muhammad UsmanPublished Date : 2021-09-13
DOI : https://doi.org/10.12982/CMUJNS.2021.087
Journal Issues : Number 4, October-December 2021
Abstract To assess the efficacy of garlic in comparison with pitavastatin in reducing hypercholesteremia. Databases that include PubMed/Medline, Cochrane, TRIP and SCOPUS were searched. All randomised controlled trials selected for the study. Studies comparing garlic with placebo and pitavastatin with either placebo or other drugs were selected to treat hypercholesteremia. Statistical analysis done using a random-effect model, and results expressed in Mean difference and variance for continuous data with 95% confidence intervals (CI). Twelve studies analysed the efficacy of garlic compared to pitavastatin. Total cholesterol, low-density lipoprotein, high-density lipoprotein, and triglycerides assessed for garlic and pitavastatin's comparative efficacy. Mean difference noticed in total cholesterol in garlic arm was -13.604 with 95% CI = -22.246, -4.962 while in pitavastatin group was -28.205 (95% CI = -29.016,-27.394). The LDL-c reduction not recorded in the garlic arm where the mean increase was recorded of 0.309 (95% CI = -12.502, 13.120) while in the pitavastatin group was -35.538 (95% CI = -39.992, -31.084). Similarly, the increase in HDL was more in the pitavastatin group 5.308 (95% CI = 0.906, 9.710 compared to garlic (2.754 with 95% CI = 1.069, 4.440). Triglycerides level reduction was also low in whereas pitavastatin was -24.210 with 95% CI = -29.249, -19.171.The analysis showed that garlic has a significant effect on lipid profile. The comparison profile of garlic with pitavastatin showed clinical application in the treatment of mild-moderate hypercholesteremia—further studies required the investigator to use the combination therapy in controlled trials.
Keywords: Allicin, Allium sativum, Dyslipidemia, Garlic, Hypercholesteremia, Hyperlipidemia Pitavastatin
Funding: The authors are appreciated for the research funding partly provided by the Chiang Mai University, Thailand.
Citation: Saeed, M.W., Gillani, S.W.*, Mahmood, R.K., and Usman, M. 2021.Assessment of the antihyperlipidemic effect of garlic vs pitavastatin in patients with moderate hyperlipidemia: A metanalysis of Randomized controlled trials. CMU J. Nat. Sci. 20(4): e2021087.
INTRODUCTION
Cardiovascular disease (CVD), a multifactorial disease, was rapidly increasing and considered one of the serious diseases that threaten human health globally. The incidence and mortality due to CVD is increasing at a high rate every year. (Timmis et al., 2020)as per who statistical update, 17.9 million people die due to cardiovascular disease. Some of the common factors that increase CVD risk are hypertension, diabetes, dyslipidemia and obesity. (“Cardiovascular Diseases,” n.d.)Dyslipidemia is the abnormal increase in the levels of low-density lipoproteins cholesterol and triglycerides and low levels of high-density lipoproteins cholesterols.it is now well established that as LDL concentration increase the risk of CVD increase and therefore considered to be the primary goal of CVD prevention and treatment. (Jung et al., 2014a) low cardiovascular risk patients should be first kept on non-pharmacological treatment and diet (Berthold, Sudhop, & Von Bergmann, 1998)
Garlic has been recommended as herbal medicine for multiple health issues for centuries. (Berthold et al., 1998) Crushing garlic activates alliinase enzymes that trigger the synthesis of allicin, and allicin inhibits cholesterol production in-vitro. Numerous forms of garlic can be found, such as extracted oil, raw garlic or powdered garlic tablets or capsules. (Aslani, Entezari, Askari, Maghsoudi, & Maracy, 2016) garlic has shown multiple benefits from antimicrobial to anticancer effects. Garlic is also helpful in gynaecological disease, toothache, arthritis and chronic cough. (Bayan, Koulivand, & Gorji, 2014; Petrovic et al., 2018)The most exciting effect of garlic in preventing and treating cardiovascular diseases and risk factors is lowering cholesterol, Blood pressure lowering, fibrinolysis stimulation, anticoagulation, and ant oxidation (Berthold et al., 1998). The mechanism of reducing hyperlipidemia by garlic achieved by suppressing low-density lipoprotein oxidation, increasing High-density lipoproteins, and decreasing triglycerides.(Gardner, Chatterjee, & Carlson, 2001; Katsuki, Hirata, & Ishikawa, n.d.; Ziaei, Hantoshzadeh, Rezasoltani, & Lamyian, 2001)
Patients at greater risk of cardiovascular events or whose hyperlipidemia is not getting controlled hypolipidemic drugs must add to their treatment.(MA1 et al., 2003) HMG CoA reductase or statins considered to be the first choice for the treatment of dyslipidemia.(Grundy et al., 2019) based on intensity stains can be divided into three categories: 1) high-intensity statins (lowering LDL-c by 50% or more) 2) moderate density (lowering LDL-c by 30% to 49%) 3) low intensity (lowering LDL-c by less than 30%).(Stone et al., 2014). High-intensity statins are the first choice for the treatment, but the treatment then shifted to moderate-intensity statins such as pitavastatin if the patient cannot tolerate high-intensity statins. As per AHA guidelines 2018, the dose of pitavastatin 2mg-4mg provide a moderate intensity effect. (Grundy et al., 2019) statins are also associated with a high risk of adverse effects. The most common adverse effect is muscles symptoms like myalgia, myopathy and, in severe cases, rhabdomyolyses. Other adverse effects include an increase in serum transaminase and a high risk of new-onset of diabetes. (Rosenson, Baker, Jacobson, Kopecky, & Parker, 2014; Thompson, Panza, Zaleski, & Taylor, 2016)
Although statins are considered first-line therapy for hyperlipidemia, a high risk of adverse events are associated with statins therapy. Therefore, it is necessary to find an alternative for treating hyperlipidemia with minor side effects and high benefits. The objective of the study is to compare the efficacy of garlic in lowering LDL-c against moderate-intensity pitavastatin.
MATERIALS AND METHODS
Criteria for considering studies for this review
Types of studies
Randomised controlled trials that recorded the clinical outcomes for garlic and pitavastatin in lowering the LDL-c in patients with hyperlipidemia or dyslipidemia were selected. RCTs, preferably cross over trials irrespective of blinding published in English language only, were included in the study. Quasi RCTs and cohort studies not included in this review. An adapted Prisma flow chart of study selection included. (Liberati et al., 2009)
Types of participants
Adults (18 years or older) of any ethnic origin that suffering from hyperlipidemia.
Diagnostic criteria
We included studies if participants were individuals with hyperlipidemia defined as a mean LDL cholesterol level between 90mg/dl to 10mg/dl and a mean TC level greater than 240 mg/dL. We accepted other definitions because the diagnostic criteria have changed during the last decade. We excluded familial hypercholesterolemia and secondary hypercholesterolemia.
Types of intervention
Garlic is available in garlic capsules, garlic powder, extracted garlic oil or raw garlic. All these forms included under one category of intervention—Pitavastatin 2 mg selected as an intervention for the control group. We removed articles having any co-interventions with the experimental group or controlled group. Trials with a minimum of 30 days of treatment duration included in the review.
Types of outcomes measures
The primary outcome measures we sought at the end of treatment and maximal follow-up after completion of the treatment were:
Primary Outcomes:
Serum cholesterol levels (including TC, LDL-c and HDL-c).
Secondary outcomes:
Triglycerides levels (TG)
Covariates, effect modifiers and confounders
- 1. Age;
- 2. Gender;
- 3. Compliance.
Timing of outcome measurement
The minimum treatment duration of treatment was one month (30 days).
Search strategy
A computer-based randomised controlled trials search was done from electronic databases PubMed, JAMA network and clinical key, using the keywords ‘GARLIC’ OR ‘ALLIVUM SATIVUM’ OR ALLICIN and ‘pitavastatin’ and hypercholesterolemia (‘Hypercholesterolemia’ OR ‘Hyperlipidemia’ OR ‘Dyslipidemia’), to get all studies published till 2019.
PubMed: search done using the above keywords mentioned above for search of articles. Filters were applied of the year from 2000 until 2021, English language and randomised controlled trials.
Cochrane: trials found using the keywords mentioned above using filters of trials from 2000 onwards with the English language.
JAMA Network: search conducted using the above keywords and with active filters of research and statins with a year range from 2000 to 2021.
Data Extraction
After selecting trails that fulfilled inclusion criteria, data relevant to population and interventions was extracted by two authors (MS, RKM) using guidelines provided by Cochrane collaboration. Any disagreement resolved by discussion or if required by a third party (SM). We sought any relevant missing information on the trial from the article's original author(s) if required.
Quality Assessment
Two authors (MS, MW) assessed each trial independently. In particular, we checked the following components: the generation of the allocation sequence; allocation concealment; blinding, and incomplete outcome data. The second version of the Cochrane Risk of Bias tool (ROB2) assessed the risk of bias for randomised controlled trials. ROB2 is a fixed set of bias domains, mainly focusing on various aspects of trial design conduct and reporting (Higgins et al., 2011). We used the following criteria.
- 1. Was the allocation sequence adequately generated?
- 2. Was the allocation adequately concealed?
- 3. Was knowledge of the allocated intervention adequately prevented during the study?
- 4. Were incomplete outcome data adequately addressed?
- 5. Dose reports of the study free of suggestion of selective outcome reporting?
- 6. Was the study free of other problems that could put it at a high risk of bias?
We used these criteria to judge the high, low or unclear risk of bias for individual bias items described in the Cochrane Handbook for Systematic Reviews of Interventions. A 'risk of bias graph' figure and 'risk of bias summary' figure are attached.
Analysis
Metanalyses conducted using the Comprehensive metanalysis software 3 (Borenstein, M., Hedges, L., Higgins, J., & Rothstein & Biostat, Englewood, 2013). The generic variance model and random effects used, owing to high heterogeneity between trials. Mean difference and standard errors between garlic and pitavastatin groups calculated at the end of the trial, with the mean difference adjusted for baseline differences between the intervention groups. The I2 statistics assessed heterogeneity. Heterogeneity was considered low if I2 < 30%, moderate if I2 = 30 – 75%, and high if I2 > 75%.Blood lipid levels collated in mg/dL. If cholesterol levels (TC, HDL, LDL) or triglyceride levels published in mmol/L, the amount multiplied by a factor of 38.7 for cholesterol and 88.6 for triglycerides to convert to mg/dL. Mean differences calculated as follows: Effect means = (end mean garlic - end mean pitavastatin) - (mean baseline garlic - mean baseline pitavastatin). Meta-analyses of all eligible trials on the effect of garlic on total cholesterol (TC), LDL cholesterol, HDL cholesterol, and triglyceride conducted by duration (4–8 weeks [short] or >8 weeks [long]), by TC baseline (
RESULTS
Description of studies:
The initial search using the electronic search strategies listed above yielded 13114. We did not include any unpublished study. After removing duplicate trials from different databases, we kept 3239 studies potentially relevant for further assessment. Out of 3239 articles, 3175 articles excluded as these studies were either reviews, cohort studies, or meetings. Twenty-six studies excluded from this study on lack of comparison, lack of required data and meta-analysis. 11 studies were selected for meta-analysis. (Superko & Krauss, 2000; Saito et al., 2002; Park et al., 2005; Gardner et al., 2007; Hak Lee et al., 2007; Kojuri, Vosoughi, & Akrami, 2007; Sobenin, Andrianova, Demidova, Gorchakova, & Orekhov, 2008; Yokote et al., 2008; Ose, Budinski, Hounslow, & Arneson, 2009; Saku, Zhang, & Noda, 2011; Higashikawa, Noda, Awaya, Ushijima, & Sugiyama, 2012; Jung et al., 2014b; Vasani, Savsani, Mehta, Bhatt, & Solanki, 2015)1 studies were a four-arm trial, but only one arm of raw garlic was included in the study(Gardner et al., 2007).
Included Studies and Participants:
A total of 2369 participants with hyperlipidemia included in 12 trials. Out of 2369, only 1009 participants included in the study. Among 1009 participants, 280 were recruited in the garlic group, while 729 included in the pitavastatin group. All studies included were in the English language. Out of 12 trials, 6 were double-blind, randomised controlled trials.(Superko & Krauss, 2000; Saito et al., 2002; Gardner et al., 2007; Sobenin et al., 2008; Ose et al., 2009; Jung et al., 2014b) 4 studies included were open-label randomized controlled trials. (Park et al., 2005; Hak Lee et al., 2007; Vasani et al., 2015; Yokote et al., 2008). There was no clarity of blinding in one randomised controlled trial. (Saku et al., 2011)
In three studies, included patients having dyslipidemia were Total cholesterol, LDL-c, and triglycerides were above their normal range.(Saito et al., 2002; Sobenin et al., 2008; Yokote et al., 2008) in the remaining studies only LDL-c was higher (Saito et al., 2002; Sobenin et al., 2008; Yokote et al., 2008).In three studies, included patients having dyslipidemia were Total cholesterol, LDL-c, and triglycerides were above their normal range.(Saito et al., 2002; Sobenin et al., 2008; Yokote et al., 2008) in the remaining studies only LDL-c was higher (Saito et al., 2002; Sobenin et al., 2008; Yokote et al., 2008).
Different formulations of garlic were used in the studies of garlic. Garlic powder used as an intervention in three studies(Superko & Krauss, 2000; Gardner et al., 2007; Sobenin et al., 2008), but the concentration of powdered garlic was different in all the trials.
In one trial, aged black garlic used as an intervention.(Jung et al., 2014b) In one study, garlic fermented with monascuspilosus used.(Higashikawa et al., 2012) One study used raw garlic as an intervention(Gardner et al., 2007). All trials reported quality standards for garlic preparation. In the remaining studies, the pitavastatin 2mg tablet used as an intervention for hyperlipidemia. (Saito et al., 2002; Park et al., 2005; Hak Lee et al., 2007; Ose et al., 2009; Saku et al., 2011; Vasani et al., 2015) the duration of intervention varied from one month to 6 months. We did not group the outcome data based on the duration of the intervention
9 out of 12 studies reported serum cholesterol levels such as total cholesterol, LDL-c, HDL-c, Triglycerides.(Superko & Krauss, 2000; Saito et al., 2002; Park et al., 2005; Hak Lee et al., 2007; Sobenin et al., 2008; Yokote et al., 2008; Higashikawa et al., 2012; Jung et al., 2014b; Vasani et al., 2015) 3 trials did not report total cholesterol levels(Gardner et al., 2007; Ose et al., 2009; Saku et al., 2011), while in one study data for HDL-c, Triglycerides was also missing(Ose et al., 2009)9 out of 12 studies reported serum cholesterol levels such as total cholesterol, LDL-c, HDL-c, Triglycerides.(Superko & Krauss, 2000; Saito et al., 2002; Park et al., 2005; Hak Lee et al., 2007; Sobenin et al., 2008; Yokote et al., 2008; Higashikawa et al., 2012; Jung et al., 2014b; Vasani et al., 2015) 3 trials did not report total cholesterol levels(Gardner et al., 2007; Ose et al., 2009; Saku et al., 2011), while in one study data for HDL-c, Triglycerides was also missing(Ose et al., 2009).
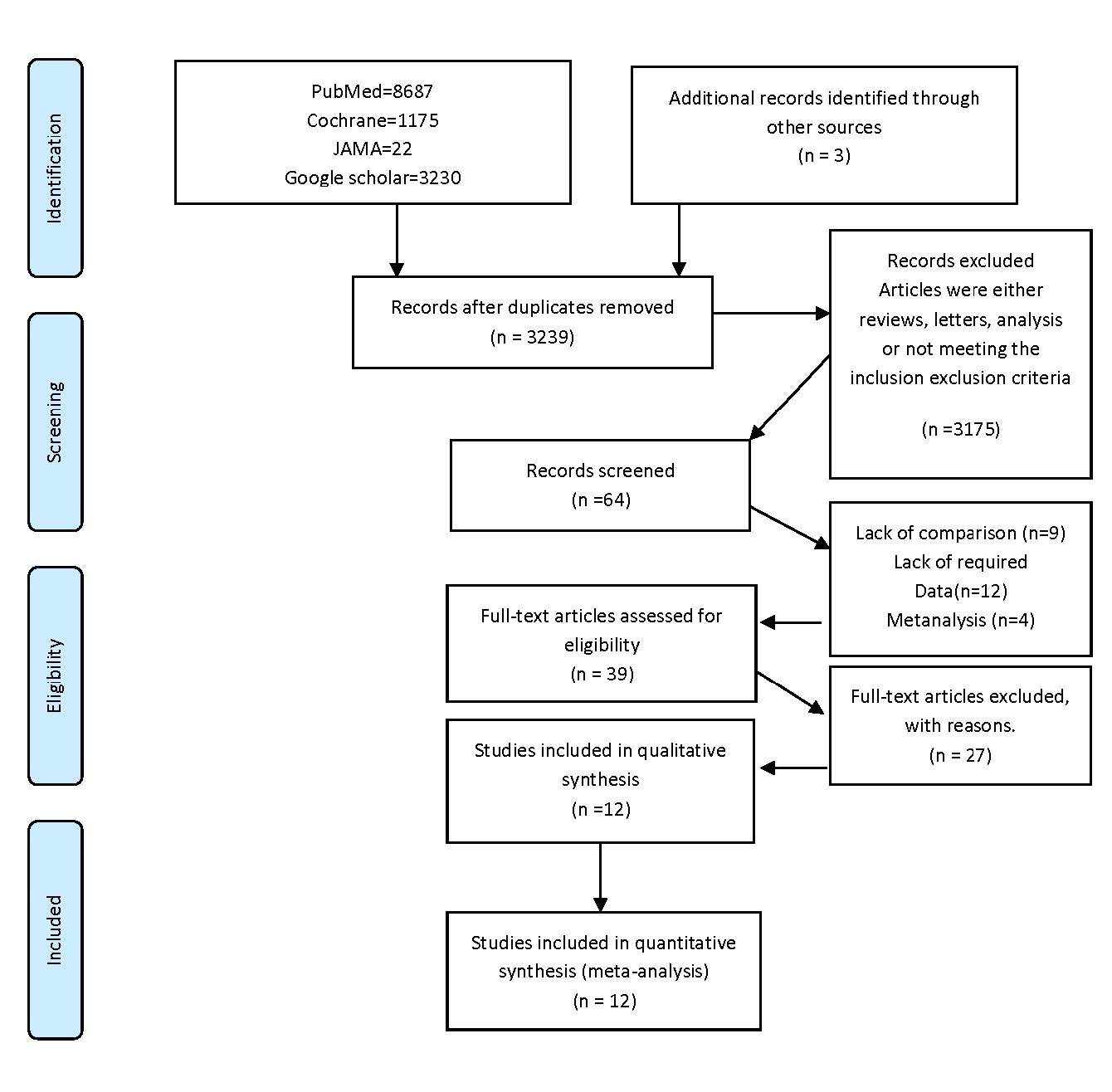
Figure 1. Prisma Flow Chart.
Table 1. Study Characteristics of meta-analysis.
|
Sr No. |
Author and Year |
Number of participants |
Study design |
intervention |
Primary outcomes |
Duration of treatment |
Conclusion |
|
1 |
Superko et al. 2000 |
50 |
A double-blind, randomised controlled trial |
1) Garlic powder 300mg three times daily 2) Placebo three times daily |
Triglycerides Total cholesterol LDL cholesterol HDL cholesterol LDL diameter (A) LDL IIIa ⫹ b% Apo B Lp(a) HDL2a% HDL2b% HDL3a% HDL3b% HDL3c% |
Three months |
No effect of garlic therapy noticed on major lipoproteins, HDL subclass Lpo(a), postprandial triglycerides. |
|
2 |
Saito et al. 2002 |
240 |
Double randomised controlled trial |
1) Pitavastatin 2mg once daily 2) Pravasatatin 10mg once daily |
TC, LDL-c TG |
Three months |
Pitavastatin found to be more effective than pravastatin in the treatment of hypercholesteremia |
|
3 |
Park et al. 2005 |
95 |
randomised open-label trial |
1) Pitavastatin 2mg once daily 2) Simvastatin 20mg once daily |
Total cholesterol Triglyceride LDL cholesterol HDL cholesterol |
Eight weeks |
The HMG-CoA reductase inhibitor pitavastatin found to be non-inferior to simvastatin in terms of reducing LDL cholesterol, total cholesterol, and triglyceride levels and increasing HDL cholesterol |
|
4 |
Gardner et al. 2007 |
169 |
Double-blind Randomised controlled trial |
1) Raw garlic 4gm once daily for six days per week 2) Garlic powder 4tablets once daily, six days per week 3) Aged garlic extract 4) Placebo tablets |
LDL-c |
Six months
|
None of the forms of garlic achieved the statistical or clinical effects on LDL–c or other lipid concentrations in moderate hyperlipidemia |
|
5 |
Lee et al. 2007 |
222 |
Open-label randomised control trial |
1) Pitavastatin 2mg once daily 2) Atorvastatin 10mg once daily |
LDL-c |
Four weeks |
No significant difference noted in the reduction of lipid profile with both drugs |
|
6 |
Sobenin et al. 2008 |
42 |
A double-blind, randomised controlled trial |
1) Powdered garlic 600mg tablet one tablet twice daily 2) Placebo one tablet twice daily |
Total cholesterol Triglyceride LDL cholesterol HDL cholesterol |
Three months |
Results demonstrated improved cardioprotective action of garlic |
|
7 |
Yokote et al. 2008 |
251 |
An open-label randomised controlled trial |
1) Pitavastatin 2mg 2) Atorvastatin 10mg |
per cent change from baseline in non-HDL-c level after 12 weeks of treatment |
Twelve weeks |
Both drugs had shown equal efficacy in reducing lipid profile |
|
8 |
Ose et al. 2009 |
843 |
A double-blind double-dummy randomised controlled trial |
1) Pitavastatin 2mg once daily 2) Pitavastatin 4mg once daily 3) Simvastatin 20mg once daily 4) Simvastatin 40mg once daily |
per cent change in LDL-c level from baseline to endpoint |
Three months |
Pitavastatin is as efficacious as simvastatin in primary hypercholesteremia as well as combined dyslipidemia |
||
|
9 |
Saku et al. 2011 |
302 |
Randomised controlled trial |
1) atorvastatin 10mg once daily 2) rosuvasttatin2.5mg once daily 3) pitavastatin 2mg once daily
|
changes in LDL-c |
4months |
The safety and efficacy of these three potent statins are equal. |
||
|
10 |
Jung et al. 2014 |
55 |
a double-blind, randomised controlled trial |
1) aged garlic 3g twice daily 2) placebo twice daily |
total cholesterol (TC), triglyceride (TG), HDL-cholesterol (HDL-c), LDL-cholesterol (LDL-c), free fatty acid (FFA), apoA1, and apoB |
Three months |
Aged black garlic reduced atherosclerotic markers in patients |
||
|
11 |
Vasani et al., 2015 |
100 |
An open-label randomised controlled trial |
1) pitavastatin 2mg once daily 2) atorvastatin 10mg once daily |
1. increase in HDL-c 2. Percent decrease in LDL-c 3. Per cent decrease in triglyceride (TG) and total cholesterol (TC) 4. Percent decrease in LDL-c: HDL-c ratio and TC: LDL-c ratio. |
Three months |
In this study, pitavastatin found to be more efficacious than atorvastatin in increasing HDL-c levels while as efficacious as atorvastatin in decreasing LDL-c in dyslipidemic patients. Atorvastatin better tolerated than pitavastatin. |
||
|
12 |
Higashikawa 2012 |
55 |
A randomised, double-blind controlled trial |
1) Fermented garlic extract with monascuspilosus900mg once daily 2) Placebo once daily |
1.Reduction in triglycerides 2. Reduction in Low-density lipoprotein 3. Reduction in total cholesterol 4. Improvement in HDL-c |
Three months |
The intake of MGFE decreased triglyceride and cholesterol in serum with no appreciable adverse effects in normal to mildly hyperlipidemic individuals, suggesting that it may be practical to improve and prevent metabolic syndrome. |
|
|
Quality Assessment:
Quality assessment was done using the ROB2 quality assessment tool.(Higgins et al., 2011) Review authors' judgements about each risk of bias item presented as percentages across all included studies in Figure 2. Figure 3 shows the review authors judgement of individual studies for different domains of risks (represented by D1 to D5) that include randomisation process deviation from intervention, missing outcomes data, measurement of outcomes data, and selection of reported results. D6 in figure 3 represents the overall risk of bias of each study. It noted that the concern was highest in the selection of reported results in three studies (Gardner 2007, Lee 2017, and Jung 2017) while the high risk was noted in the study, Saito 2002. One study Vasani 2015 was having risk risk as a high risk of bias noted in the randomisation process as well as the outcome measurements.
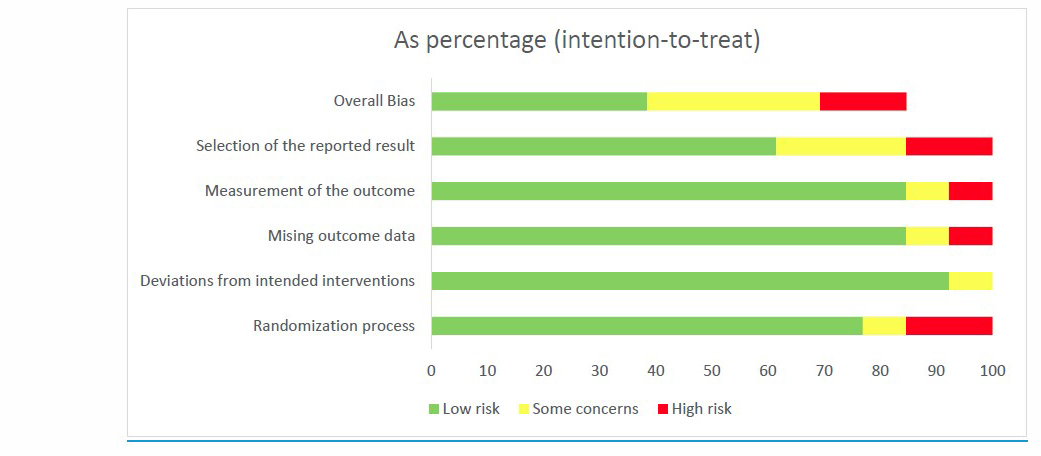
Figure 2. Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.
Total eight studies recorded total cholesterol, four from the garlic group and four from the pitavastatin group. The analysis showed that although there was the effect of garlic on total cholesterol but was insignificant when compared to the pitavastatin group. The mean difference noted in the garlic group was -13.604 with 95% CI = -22.246, -4.962, whereas, in a group of pitavastatin, the total mean -28.205 (95% CI = -29.016,-27.394). (Figure 4) Analysis conducted using random effects. We did the within-group analysis to evaluate reason heterogeneity, and figure A.1 represents the funnel plot by removing studies with publication bias reduced heterogeneity.
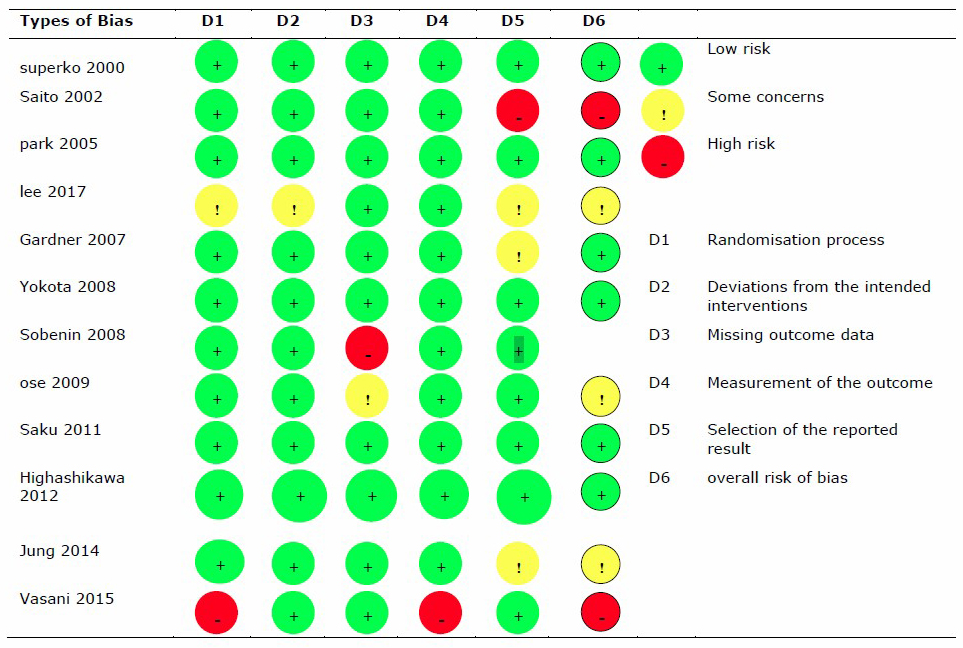
Figure 3. Quality Assessment of Randomized Controlled trials included in the meta-analysis.
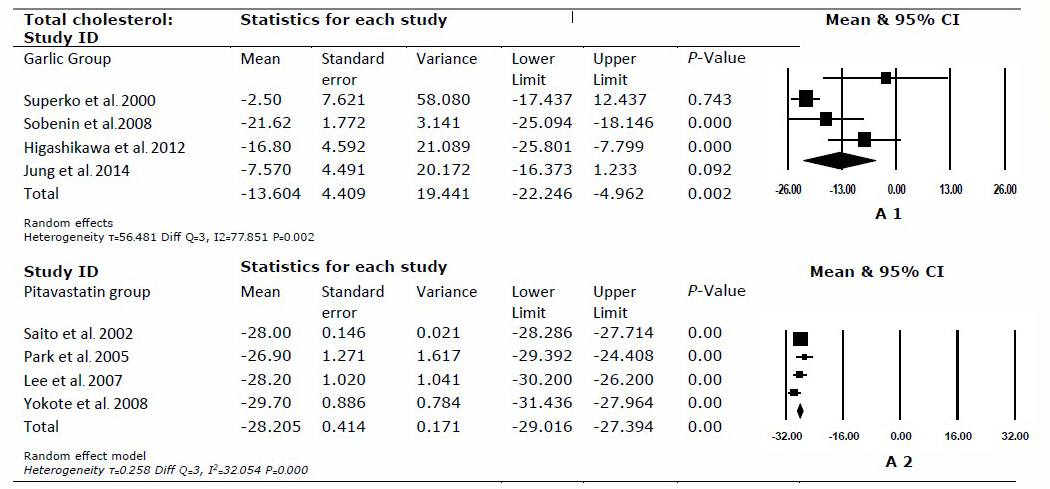
Figure 4. Shows the forest plot for garlic and pitavastatin group in lowering total cholesterol. The black box represents the mean, and its size presents the weight of the study; the black line represents a 95% CI interval.
Low-Density Lipoprotein:
Low-density lipoprotein was recorded in five studies garlic groups, while seven studies in the pitavastatin group included in the analysis of low-density lipoprotein. Garlic found to have no significant effect as the mean of the garlic group 0.309 (95% CI = -12.502, 13.120). In pitavastatin group the total mean was -35.538 (95% CI = -39.992, -31.084). (Figure 5) The total mean pitavastatin group found to be significantly higher than the garlic group. Analysis was done within the group to evaluate heterogeneity. Figure B 1 and B 2 represent funnel plots after removing studies with publication bias showing a reduction in heterogeneity.
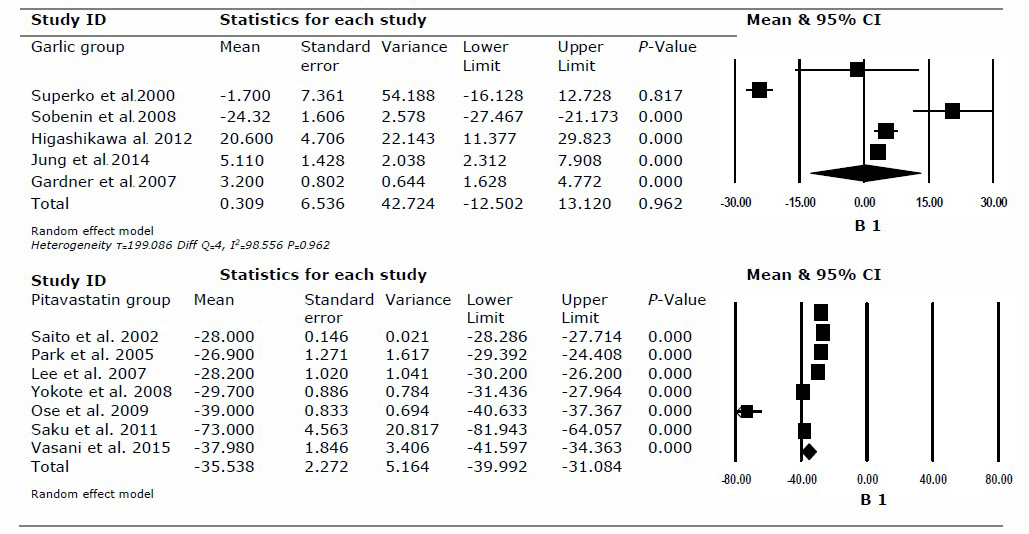
Figure 5. Shows the forest plot for garlic and pitavastatin group in lowering low-density lipoprotein. The black box represents the mean, and its size presents the weight of the study; the black line represents a 95% CI interval.
High-Density lipoprotein:
Total 11 studies included in the analysis of High-density lipoprotein, five studies for the garlic arm, while six studies for the pitavastatin group. Analysis showed increase in high-density lipoprotein in both arms. The total mean increase of high-density lipoprotein in garlic recorded 2.754 with 95% CI = 1.069, 4.440, while the total mean in the pitavastatin group is 5.308 (95% CI = 0.906, 9.710). (Figure 6) Analysis was done within the group to evaluate heterogeneity figure C 1 and C 2. representing funnel plots after removal of studies with publication bias showing the reduction in heterogeneity.
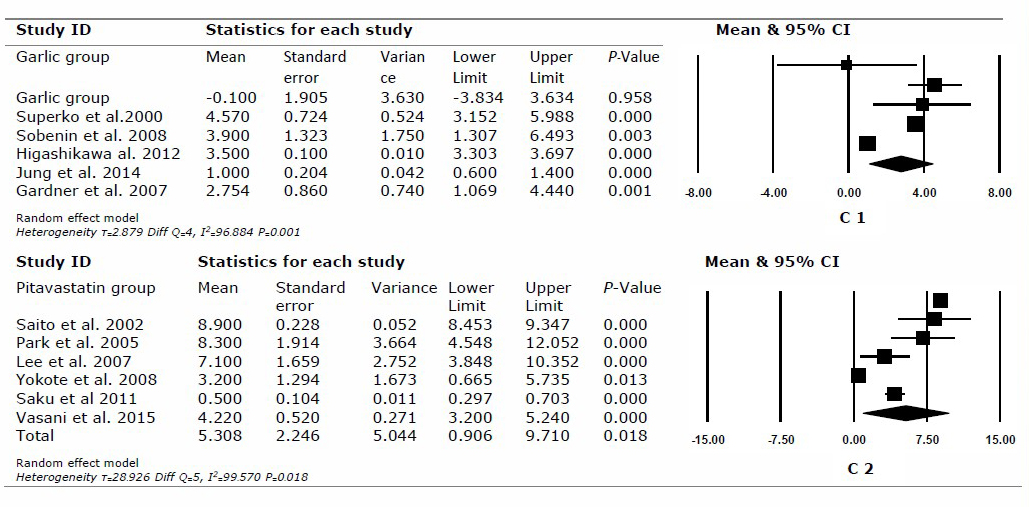
Figure 6. Shows the forest plot for garlic and pitavastatin group in increasing high-density lipoprotein. The black box represents the mean, and its size presents the weight of the study; the black line represents a 95% CI interval.
Triglycerides:
Eleven studies assessed for the analysis of triglycerides, five in the garlic group and six in the pitavastatin group. The total mean decrease in garlic noted was -9.839 (95% CI = -18.260, -1.417). The decrease of triglycerides in the pitavastatin group was significantly high, where the mean decrease noted was -24.210 with 95% CI = -29.249, -19.171. Pitavastatin found to superior in reducing triglycerides than garlic. (Figure 7) Within-group analysis done for evaluation of reasons for heterogeneity. Figure A 2. showing funnel plot after removal of studies with publication bias thereby, reducing heterogeneity. Within-group analysis of the pitavastatin group was not possible as only two studies remain after removing biased studies.
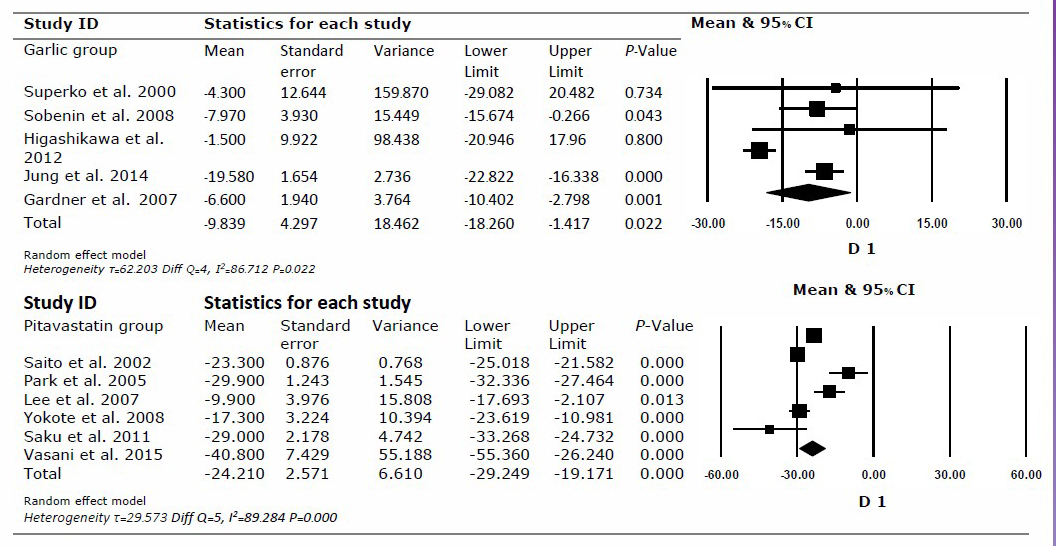
Figure 7. Shows the forest plot for garlic and pitavastatin group in lowering triglycerides. BlackThe black box representrepresents the mean, and its size presents the weight of the study, balck; the black line representrepresents a 95% CI interval.
DISCUSSION
The current comparative study investigated the effects of garlic in lowering the serum cholesterol during 1 to 4 months of treatment in patients with moderate hyperlipidemia—a group receiving pitavastatin considered a positive control. The study's main findings were that although garlic showed a reduction in total cholesterol and triglycerides, it was not significantly high compared with pitavastatin. High heterogeneity is noticed, possibly due to different garlic formulations at different doses and for different durations.
Several meta-analyses supported the cholesterol-lowering activity of garlic.(“Garlic as a Lipid Lowering Agent--a Meta-Analysis - PubMed,” n.d.; Sun, Wang, & Qin, 2018; Warshafsky, Kamer, & Sivak, 1993; Zeng et al., 2012) while some meta-analyses reported no activity of garlic on serum cholesterol reduction that may be due to the loss of active compound during the processing.( Stevinson, Pittler, & Ernst, 2000; Reinhart, Talati, White, & Coleman, 2009; Ried, Toben, & Fakler, 2013). Although one randomised controlled trial conducted on a comparison of garlic and atorvastatin in reducing c reactive protein and lipid profile, the results showed no significant difference compared with atorvastatin. (van Doorn et al., 2006) The analysis conducted using randomised controlled trials that published in the year 2000 and onwards.
Garlic may reduce the absorption of cholesterol and synthesis of cholesterol and fatty acid, thereby reducing the level of cholesterol. (Isaacsohn et al., 1998) this reduction is due to the presence of compound allicin in garlic that leads to the reduction of cholesterol. (Lawson & Wang, 2001). Several different forms of garlic used in the studies included raw garlic, powdered garlic, and garlic extract. The subgroup analysis was not possible due to the low quality of data retrieved from included studies.
The analysis showed that Total cholesterol reduction noted in both groups, but in comparison to the pitavastatin group, the reduction in the garlic group was not significant. The significant difference showed that pitavastatin is more effective in reducing total cholesterol compared with garlic. The variance found to be very high in three studies of the garlic group, indicating high heterogeneity probably among trial participants. (Superko & Krauss, 2000; Higashikawa et al., 2012; Jung et al., 2014b) High heterogeneity has made the resulting conservative; if we remove the studies with high heterogeneity, the mean reduction of total cholesterol in the garlic group comes down to -10. Thus, showing garlic effect in reducing total cholesterol has been reduced by 2. (Figure A1). One trial and two meta-analyses support the reduction of total cholesterol by garlic, but so far, no group compared garlic with mild to moderate antihyperlipidemic. (Warshafsky et al., 1993; Zeng et al., 2012; Sun et al., 2018) one clinical trial that compared garlic with atorvastatin 40mg found garlic was not statistically significant to atorvastatin in reducing total cholesterol.(van Doorn et al., 2006)
Garlic showed no effect on lowering low-density lipoprotein. Low-density lipoprotein found an increase in the garlic group instead of decreasing. At the same time, the pitavastatin group has shown a significant effect with a mean reduction of low-density lipoprotein -35. Variance in garlic was high in two studies that show high heterogeneity. (Superko & Krauss, 2000; Higashikawa et al., 2012) High heterogeneity may limit the result. After removing studies with high heterogeneity, the difference in mean reduction between garlic and pitavastatin groups was almost similar. (Figure B1, figure B2) One metanalysis supports the reduction of low-density lipoprotein by garlic (Sun et al., 2018), but so far, the reduction has not noticed in current analysis. While three meta-analyses supported the study, no appreciable reduction noted in low-density lipoprotein with garlic.(Reinhart et al., 2009; Stevinson et al., 2000; Zeng et al., 2012)
High-density lipoprotein found to improve with both garlic and pitavastatin, but pitavastatin found to have a significant effect on garlic when a comparison made. The variance was low in both garlic and pitavastatin groups. High heterogeneity noted in both groups. After removing studies with high heterogeneity, subgroup analysis showed that the total mean difference increase of HDL with garlic was higher by one. One meta-analysis recorded an improvement of high-density lipoprotein with garlic. (Zeng et al., 2012) two meta-analyses have not recorded any improvement in high-density lipoprotein. (Ried et al., 2013; Sun et al., 2018)
Triglycerides reduction with garlic when compared with pitavastatin found to have an insignificant effect. The reduction of triglycerides with pitavastatin was almost three times that was reduced by garlic. Analysis again recorded high variance in three studies of garlic, indicating high heterogeneity possibly due to trial patients. Studies with high heterogeneity removed in subgroup analysis and forest plots showed less triglyceride reduction with garlic. (Figure D1) Only one meta-analysis supports the current analysis of garlic in reducing triglycerides (“Garlic as a Lipid Lowering Agent--a Meta-Analysis - PubMed,” n.d.), but the remaining meta-analysis found no significant difference in the reduction of triglycerides with garlic. ( Warshafsky et al., 1993; Alder, Lookinland, Berry, & Williams, 2003; Khoo & Aziz, 2009; Ried et al., 2013; Sun et al., 2018)
The pooled analysis of the comparison inefficacy of garlic, compared with pitavastatin, has shown that although garlic has shown results in the reduction of total cholesterol and triglycerides but not enough when compared with pitavastatin. The pooled analysis has also shown that increase in HDL-c level was much high with pitavastatin. The difference in total cholesterol reduction between pitavastatin and garlic was more significant than 14 mg/dL at the end of therapy. Similarly, pooled analysis of LDL-c also supported pitavastatin against garlic in reducing the LDL-c concentration. The mean difference in reducing LDL-c between pitavastatin and garlic found to be more than 35mg/dL, which signifies that pitavastatin is far superior to garlic.
Improvement in HDL-c levels was higher in the pitavastatin group in comparison to garlic. The pooled analysis showed that improvement in HDL-c concentration was twice as high in patients taking pitavastatin than patients taking garlic. Reduction in triglycerides was also significant in the pitavastatin group compared to the garlic group, where the mean difference was 15mg/dL.
It can argue that the results show in our studies cannot be implemented in the high-risk cardiovascular group—patients whose serum lipids levels are above borderline or having mild hypocholesteremia. Garlic found to have a little hypolipidemic effect. The quality of studies included also has restricted the implementation of the results. Several study design issues noted in the meta-analysis studies, like the randomisation process not mentioned in some studies.
Limitations:
- In this meta-analysis, the newer studies included published after 2000 instead of old ones that reported little or no beneficial effect of garlic on all serum cholesterol outcomes measures.
- High heterogeneity among studies is of concern as it shows the potential presence of confounding factors. Such confounding factors like some trials applied dietary and lifestyle modification while some did not. In this review, we did not attempt a subgroup analysis with or without such restrictions due to inconsistencies in the restrictions applied in trials.
- The quality of studies also found to be of deep concern concerning study design, reporting and methodology. Out of twelve studies, four found to have complete details of their study design. (Superko & Krauss, 2000; Yokote et al., 2008; Saku et al., 2011; Higashikawa et al., 2012)
- The quality of studies also found to be of serious concern concerning study design, reporting and methodology. Out of twelve studies, four found to have complete details of their study design. (Superko & Krauss, 2000; Yokote et al., 2008; Saku et al., 2011; Higashikawa et al., 2012)
- So far, no randomised controlled trial conducted for comparison of garlic with HMG-CoA reductase inhibitors in mild to moderate antihyperlipidemic activity.
- Many studies included in the garlic group were of small Sample Size.
CONCLUSION
The evidence suggests that garlic has a significant effect on lipid profile, but pitavastatin is far superior in reducing total cholesterol, LDL-c, and triglycerides and improving HDL-c levels. Garlic cannot use as an alternative to pitavastatin in moderate hyperlipidemia. As garlic has shown to reduce total cholesterol and triglycerides, we can consider that it can be given in combination with pitavastatin or other HMG-CoA reductase inhibitors far, no comparative done in which garlic compared to any mild to moderate hypercholesteremia. Further evaluation is needed to assess the efficacy of garlic either in combination with HMG-CoA reductase inhibitors to treat mild-moderate hypercholesteremia.
REFERENCES
Alder, R., Lookinland, S., Berry, J.A., and Williams, M. 2003. A systematic review of the effectiveness of garlic as an anti-hyperlipidemic agent. Journal of the American Academy of Nurse Practitioners. 15: 120–129.
Aslani, N., Entezari, M.H., Askari, G., Maghsoudi, Z., and Maracy, M.R. 2016. Effect of garlic and lemon juice mixture on lipid profile and some cardiovascular risk factors in people 30-60 years old with moderate hyperlipidaemia: A randomized clinical trial. International Journal of Preventive Medicine, 2016-JULY.
Bayan, L., Koulivand, P.H., and Gorji, A. 2014. Garlic: a review of potential therapeutic effects. Avicenna Journal of Phytomedicine. 4: 1–14.
Berthold, H.K., Sudhop, T., and Von Bergmann, K. 1998. Effect of a garlic oil preparation on serum lipoproteins and cholesterol metabolism: A randomized controlled trial. Journal of the American Medical Association. 279: 1900–1902.
Borenstein, M., Hedges, L., Higgins, J., Rothstein, H., and Biostat, Englewood, N. 2013. Comprehensive Meta-Analysis Version 3, 2013.
Cardiovascular diseases. (n.d.). Retrieved March 10, 2021, from https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1
Gardner, C.D., Chatterjee, L.M., and Carlson, J.J. 2001. The effect of a garlic preparation on plasma lipid levels in moderately hypercholesterolemic adults. Atherosclerosis, 154: 213–220.
Gardner, C.D., Lawson, L.D., Block, E., Chatterjee, L.M., Kiazand, A., Balise, R.R., and Kraemer, H.C. 2007. Effect of raw garlic vs commercial garlic supplements on plasma lipid concentrations in adults with moderate hypercholesterolemia: A randomized clinical trial. Archives of Internal Medicine. 167: 346–353.
Garlic as a lipid lowering agent--a meta-analysis - PubMed. (n.d.). Retrieved April 11, 2021, from https://pubmed.ncbi.nlm.nih.gov/8169881/
Grundy, S.M., Stone, N.J., Bailey, A.L., Beam, C., Birtcher, K.K., Blumenthal, R.S., … Yeboah, J. 2019. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/
NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation, Vol. 139, pp. E1082–E1143. Lippincott Williams and Wilkins.
Hak Lee, S., Chung, N., Kwan, J., Kim, D. Il, Ho Kim, W., Jeong Kim, C., … Su Hyon, M. 2007. Comparison of the efficacy and tolerability of pitavastatin and atorvastatin: An 8-week, multicenter, randomized, open-label, dose-titration study in korean patients with hypercholesterolemia. Clinical Therapeutics. 29: 2365–2373.
Higashikawa, F., Noda, M., Awaya, T., Ushijima, M., and Sugiyama, M. 2012. Reduction of serum lipids by the intake of the extract of garlic fermented with Monascus pilosus: A randomized, double-blind, placebo-controlled clinical trial. Clinical Nutrition. 31: 261–266.
Higgins, J.P.T., Altman, D.G., Gøtzsche, P.C., Jüni, P., Moher, D., Oxman, A.D., … Sterne, J.A.C. 2011. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ (Online), 343(7829).
Isaacsohn, J.L., Moser, M., Stein, E.A., Dudley, K., Davey, J.A., Liskov, E., and Black, H.R. 1998. Garlic powder and plasma lipids and lipoproteins: A multicenter, randomized, placebo-controlled trial. Archives of Internal Medicine. 158: 1189–1194.
Jung, E.S., Park, S.H., Choi, E.K., Ryu, B.H., Park, B.H., Kim, D.S., … Chae, S.W. 2014a. Reduction of blood lipid parameters by a 12-wk supplementation of aged black garlic: A randomized controlled trial. Nutrition. 30: 1034–1039.
Jung, E.S., Park, S.H., Choi, E.K., Ryu, B.H., Park, B.H., Kim, D.S., … Chae, S.W. 2014b. Reduction of blood lipid parameters by a 12-wk supplementation of aged black garlic: A randomized controlled trial. Nutrition. 30: 1034–1039.
Katsuki, T., Hirata, K., and Ishikawa, H. (n.d.). Significance of Garlic and Its Constituents in Cancer and Cardiovascular Disease. Retrieved from https://www.researchgate.net/publication/237264885
Khoo, Y.S.K. and Aziz, Z. 2009. Garlic supplementation and serum cholesterol: A meta-analysis. Journal of Clinical Pharmacy and Therapeutics. 34: 133–145.
Kojuri, J., Vosoughi, A.R., and Akrami, M. 2007. Effects of anethum graveolens and garlic on lipid profile in hyperlipidemic patients. Lipids in Health and Disease, 6.
Lawson, L.D., and Wang, Z.J. 2001. Low allicin release from garlic supplements: A major problem due to the sensitivities of alliinase activity. Journal of Agricultural and Food Chemistry. 49: 2592–2599.
Liberati, A., Altman, D.G., Tetzlaff, J., Mulrow, C., Gøtzsche, P.C., Ioannidis, J.P.A., … Moher, D. 2009. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Medicine. 6: e1000100.
MA1, A.P., MD2, T.H., RD3, R.L.Bs., RD3, R.A. Ms., RD3, M.R. Bs., and MD4, and Y.B. 2003. Effect of Garlic on Lipid Profile and Psychopathologic Parameters in People with Mild to Moderate Hypercholesterolemia. Retrieved March 13, 2021, from the israel medical association journal website: https://www.ima.org.il/FilesUploadPublic/IMAJ/0/54/27282.pdf
Ose, L., Budinski, D., Hounslow, N., and Arneson, V. 2009. Comparison of pitavastatin with simvastatin in primary hypercholesterolaemia or combined dyslipidaemia. Current Medical Research and Opinion. 25: 2755–2764.
Park, S., Kang, H.J., Rim, S.J., Ha, J.W., Oh, B.H., Chung, N., and Cho, S.Y. 2005. A randomized, open-label study to evaluate the efficacy and safety of pitavastatin compared with simvastatin in Korean patients with hypercholesterolemia. Clinical Therapeutics. 27: 1074–1082.
Petrovic, V., Nepal, A., Olaisen, C., Bachke, S., Hira, J., Søgaard, C. K., … Otterlei, M. 2018. Anti-cancer potential of homemade fresh garlic extract is related to increased endoplasmic reticulum stress. Nutrients. 10.
Reinhart, K.M., Talati, R., White, C.M., and Coleman, C.I. 2009. The impact of garlic on lipid parameters: A systematic review and meta-analysis. Nutrition Research Reviews. 22: 39–48.
Ried, K., Toben, C., and Fakler, P. 2013. Effect of garlic on serum lipids: An updated meta-analysis. Nutrition Reviews. 71: 282–299.
Rosenson, R.S., Baker, S.K., Jacobson, T.A., Kopecky, S.L., and Parker, B.A. 2014. An assessment by the statin muscle safety task force: 2014 update. Journal of Clinical Lipidology. 8: S58–S71.
Saito, Y., Yamada, N., Teramoto, T., Itakura, H., Hata, Y., Nakaya, N., … Goto, Y. 2002. A randomized, double-blind trial comparing the efficacy and safety of pitavastatin versus pravastatin in patients with primary hypercholesterolemia. Atherosclerosis. 162: 373–379.
Saku, K., Zhang, B., and Noda, K. 2011. Randomized head-to-head comparison of pitavastatin, atorvastatin, and rosuvastatin for safety and efficacy (quantity and quality of LDL) - The PATROL trial-. Circulation Journal. 75: 1493–1505.
Sobenin, I.A., Andrianova, I.V., Demidova, O.N., Gorchakova, T.V., and Orekhov, A.N. 2008. Lipid-lowering effects of time-released garlic powder tablets in double-blinded placebo-controlled randomized study. Journal of Atherosclerosis and Thrombosis. 15: 334–338.
Stevinson, C., Pittler, M.H., and Ernst, E. 2000. Garlic for treating hypercholesterolemia: A meta-analysis of randomize clinical trials. Annals of Internal Medicine. 133.
Stone, N.J., Robinson, J.G., Lichtenstein, A.H., Bairey Merz, C.N., Blum, C.B., Eckel, R. H., … Wilson, P.W.F. 2014. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the american college of cardiology/american heart association task force on practice guidelines. Circulation, Vol. 129, pp. 1–45. Lippincott Williams and Wilkins.
Sun, Y.E., Wang, W., and Qin, J. 2018. Anti-hyperlipidemia of garlic by reducing the level of total cholesterol and low-density lipoprotein. Medicine (United States), Vol. 97. Lippincott Williams and Wilkins.
Superko, H.R., and Krauss, R.M. 2000. Garlic powder, effect on plasma lipids, postprandial lipemia, low- density lipoprotein particle size, high-density lipoprotein subclass distribution and lipoprotein (a). Journal of the American College of Cardiology. 35: 321–326.
Thompson, P. D., Panza, G., Zaleski, A., and Taylor, B. 2016. Statin-associated side effects. Journal of the American College of Cardiology, Vol. 67, pp. 2395–2410. Elsevier USA.
Timmis, A., Townsend, N., Gale, C.P., Torbica, A., Lettino, M., Petersen, S.E., … Bardinet, I. 2020. European Society of Cardiology: Cardiovascular Disease Statistics 2019. European Heart Journal. 41: 12–85.
van Doorn, M.B., Santo, S.M.E., Meijer, P., Kamerling, I.M., Schoemaker, R.C., Dirsch, V., … Burggraaf, J. 2006. Effect of garlic powder on C-reactive protein and plasma lipids in overweight and smoking subjects. The American Journal of Clinical Nutrition. 84: 1324–1329.
Vasani, P., Savsani, D., Mehta, D., Bhatt, P., and Solanki, S. 2015. A comparative study of efficacy and safety of pitavastatin versus atorvastatin in the patients of dyslipidemia in medicine department of a tertiary care teaching hospital. International Journal of Basic & Clinical Pharmacology. 4: 24.
Warshafsky, S., Kamer, R.S., and Sivak, S.L. 1993. Effect of garlic on total serum cholesterol: A meta-analysis. Annals of Internal Medicine. 119: 599–605.
Yokote, K., Bujo, H., Hanaoka, H., Shinomiya, M., Mikami, K., Miyashita, Y., … Saito, Y. 2008. Multicenter collaborative randomized parallel group comparative study of pitavastatin and atorvastatin in Japanese hypercholesterolemic patients. Collaborative study on hypercholesterolemia drug intervention and their benefits for atherosclerosis preventi. Atherosclerosis. 201: 345–352.
Zeng, T., Guo, F.F., Zhang, C.L., Song, F.Y., Zhao, X.L., and Xie, K.Q. 2012. A meta-analysis of randomized, double-blind, placebo-controlled trials for the effects of garlic on serum lipid profiles. Journal of the Science of Food and Agriculture. 92: 1892–1902.
Ziaei, S., Hantoshzadeh, S., Rezasoltani, P., and Lamyian, M. 2001. The effect of garlic tablet on plasma lipids and platelet aggregation in nulliparous pregnants at high risk of preeclampsia. European Journal of Obstetrics and Gynecology and Reproductive Biology. 99: 201–206.
OPEN access freely available online
Chiang Mai University Journal of Natural Sciences [ISSN 16851994]
Chiang Mai University, Thailand
https://cmuj.cmu.ac.th
Muhammad Waqas Saeed1, 2 , Syed Wasif Gillani2,*, Rana Kamran Mahmood3, and Muhammad Usman4
1 Rashid Hospital, Clinical pharmacy, Dubai, Dubai, United Arab Emirates
2 Department of Pharmacy Practice, College of Pharmacy Gulf Medical University, Ajmanm UAE
3 Response plus medical - Clinical pharmacy, Abu Dhabi, United Arab Emirates
4 AL Qassimi Hospital for Women and Children – Pharmacy, Sharjah, United Arab Emirates
Corresponding author: Syed Wasif Gillani, E-mail: dr.syedwasif@gmu.ac.ae
Total Article Views
Editor: Veerasak Punyapornwithaya,
Chiang Mai University, Thailand
Article history:
Received: May 25, 2021;
Revised: July 8, 2021;
Accepted: July 22, 2021;