 ISSN: 2822-0838 Online
ISSN: 2822-0838 Online

Respiratory Health Implications among Wet-Blue Leather Tannery Workers of Kasur
Irfan Saleem, Zulfiqar Ali*, and Ali HussainPublished Date : 2021-04-01
DOI : https://doi.org/10.12982/CMUJNS.2021.058
Journal Issues : Number 3, July-September 2021
Abstract Work-related respiratory diseases have imperative role in the globular burden of occupational lung diseases throughout the world. These respiratory disorders can be caused by environmental hazards in the workplace and account for 10-20% of all chronic lung diseases. It is surprising that in Pakistan, scarce data is available on the pulmonary health of tannery workers. Therefore, this study aimed to determine the respiratory-specific health status of wet-blue leather tannery workers in Kasur city, Pakistan. A sample of 227 tannery workers engaged in four different tanneries was selected as a sample of convenience. A control group of 112 participants independent from exposure was also selected from the local community. Respiratory health was determined through an adopted symptom-based questionnaire and pulmonary function tests (PFTs). These tests were carried out by using a portable spirometer, during September-December 2019. A multiple Linear regression analysis was performed to analyze the amount of variance in PFTs by demographics and respiratory symptoms. Among tannery workers, the complaints of respiratory symptoms were 27.8% as compared to 21.4% of the control group. While based on the PFTs, total cases of impaired- pulmonary function among tannery workers were 34.3% as compared to 19.7% of the control. A statistically significant relationship was found between age, job duration, education, respiratory symptoms, and pulmonary function parameters. This study will contribute to generate baseline data of respiratory health status of the tannery workers. Further studies are recommended to find an association between occupational factors and workplace-related respiratory problems to reduce the burden of occupational diseases.
Keywords: Occupational diseases, Lung diseases, Respiratory function tests, Spirometry, Workplace
Citation: Saleem, I., Ali, Z., and Hussain, H. 2021. respiratory health implications among wet-blue leather tannery workers of Kasur. CMUJ. Nat. Sci. 20(3): e2021058.
INTRODUCTION
Work-related respiratory diseases make major contributions to the globular burden of occupational lung diseases throughout the world. It accounts for 10-20% of all chronic lung diseases (Dalju et al., 2019). The structural attributes of the lungs i.e. high vascularity, thin epithelium of alveoli, and the large surface area of the lung make it prone to the cruelty of environmental pollutants, especially in the workplace. The exposure to the workplace environment takes years; therefore, workplace-related diseases are mostly preventable (Chandrasekaran et al., 2014).
Tanning operations during leather manufacturing are constant hazards to the workers (Issever et al., 2007). Wet-blue leather produces through a chrome tanning procedure (Abbas et al., 2017). Approximately 90% of raw hides are being treated by this method (Thanikaivelan et al., 2004). Such chromium exposure has a potential effect to reduce spirometric measurements among workers (Rasoul et al., 2017). Similarly, buffing as well as loading hides in rotating- drums produce chemical and leather dust comprise microfungi, hair fragments, and excrements, etc. These dusts are related to potential hazards and involve in occupational diseases (Issever et al., 2007).
Occupational health is still at the juvenile stage in Pakistan. The tannery workers are constantly facing exposures to carcinogenic chemicals like chromium salt, benzene, formaldehyde, as well as airborne leather dust produced during different activities of tanning procedure. Such exposures are serious health threats to the tannery workers (Jamal et al., 2017). Keeping in view the toxicity of different compounds and vulnerability of the workers to respiratory disorders, the present research was conducted to study respiratory symptoms along with impaired pulmonary functions among tannery workers. Thus we can bring to prominence the decline of pulmonary functions, especially with increasing years of exposure to leather dust.
MATERIALS AND METHODS
Study area
The present study was conducted in the industrial complex of Deen Garh, Kasur city, Pakistan. The study was carried out during September-December 2019. The sample size was calculated using the G Power formula proposed by Faul et al., (2007). A total of 227 tannery workers participated from four different tanneries while 112 individuals of the control group participated from the local community; unexposed to the environment of tannery. The available workers were the only male.
Inclusion criteria
The inclusion criterion for tannery workers and control group was as directly engaged with the wet-blue leather tanning process and independence from direct-exposure, respectively.
Anthropometric measurements
Age (years), height (cm), weight (kg), and body mass index (BMI in kg/m2) were measured from studied population. To measure height, workers asked to straighten their back and head. A spring-weighing scale recorded the weight. All participants were wearing light clothes and without shoes during anthropometric measurements and pulmonary function tests (PFTs). Besides, demographic factors like sex, age, marital status, education, job duration, the use of face mask, smoking status, and ethnicity were also noted.
Symptom-based questionnaire
A symptom-based questionnaire was employed and adopted to record the status of respiratory signs and symptoms (Jamal et al., 2017). These respiratory signs and symptoms were: wheezing, chest tightness, difficulty in breathing, excessive cough, and dyspnea. However, skin allergy i.e. sneezing, nasal discharge, and eye irritation along with atopy: eczema, and urticaria were studied. The diagnosis of bronchial asthma was based on the information provided by the workers. The questionnaire was filled through face to face interviews.
Pulmonary Function Tests
PFTs were performed by using a portable spirometer (Spirotron MDX, USA). All measurements were taken by the method of the American College of Occupational and Environmental Medicine (Townsend et al., 2000) and (ATS/ERS 2005 guidelines) adopted by Viegas et al., (2013). All workers were sitting in a comfortable position during PFTs. Nose clips were used to avoid any leakage from the nose. Disposable mouth-pieces were used to avoid contamination. Self-demonstration was provided on how to exhale air forcefully during the procedure after taking a deep breath. Workers were asked to repeat the test if not performing appropriately. Three readings were taken and the highest value was selected for the analysis.
Pulmonary function parameters
Three pulmonary function parameters were recorded as forced vital capacity (FVC), forced expiratory volume in one second (FEV1), and the ratio of FEV1/FVC. The values were taken as percentage predicted for FEV1 and FVC.
Impaired pulmonary function
Impaired pulmonary function was determined in terms of the patterns of respiratory abnormalities, i.e. airflow obstruction, restriction, and mixed abnormality (co-existing airway obstruction and restriction). These patterns of abnormalities were based on the prescribed values of pulmonary function parameters (Bellamy et al., 2005). The normal pattern was indicated if the percentage predicted values of FEV1 and FVC > 80% without considering the values of FEV1/FVC. The restrictive pattern had the values of both FEV1 and FVC < 80% but FEV1/FVC > 0.7. The obstructive pattern had values of FEV1 less than 80%, FVC is usually reduced, but to a lesser extent than FEV1 while FEV1/FVC
Data analysis
Data were analyzed statistically using SPSS (version 25). Point biserial correlation was determined between pulmonary function parameters and some demographic factors of dichotomous nature. Spearman’s rho correlation was used to measure the strength and direction of association between pulmonary function parameters and some demographic factors acting as ordinal variables. The P-value of up to 0.05 was considered statistically significant. A multiple Linear regression model i.e., y = av + bw + cx +dy + ez was run to predict the variance of pulmonary function parameters by selected independent variables in terms of F and P value.
RESULTS
The demographic characteristics, respiratory symptoms, pulmonary function parameters as well as patterns of respiratory abnormalities of the studied population (n = 339) were analyzed by frequency distribution. Each category was further sub- divided to analyze their percentage frequency.
In demographic features, the gender of the studied population was only male (n = 339). There were no female participants among tannery workers and control group. The age range was recorded in four subgroups of years: < = 25, 26-35, 36-45, and > 45. The maximum tannery workers fell in a subgroup of 26-35 (34.4%) as compared to the participants of the control group fall in a subgroup of > 45 (54.5%). It was observed that most of the tannery workers and participants of the control group were married. The education was observed at three levels: <= 5 years, 6-12 years, and > 12 years. Most of the tannery workers reported <= 5 years of education (67.8%) as compared to >12 (59.8%) in the control group. The job duration was recorded in three subgroups: <= 3 years, 4-10 years, and > 10 years. Most of the tannery workers had job duration <= 3 years (65.6%) than > 10 (49.1%) in the control group. The majority of the tannery workers reported that they use face mask (53.3%) during the hours of duty. BMI was recorded in two subgroups: < = 25 and > 25. Most of the tannery workers and participants of the control group were fall in the subgroup of > 25. Similarly, the majority of the studied population reported that they never smoked. Finally, the ethnicity of the participants was observed for Urdu, Pashto, Punjabi, and miscellaneous. Most of the tannery workers were Pashto speaking (42.7%) while in the control group, Punjabi speaking (57.1%) were dominant (Table 1).
Table 1. Demographic factors among studied population.

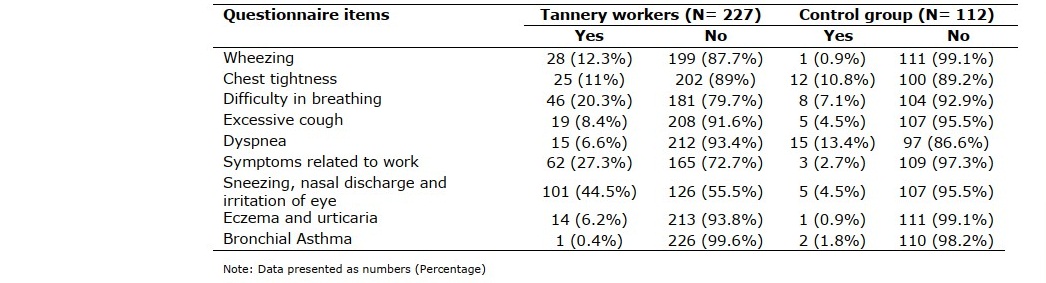
The obtained results of the symptom-based questionnaire showed that frequently reported symptom among tannery workers was difficulty in breathing (20.3%) while dyspnea (13.4%) in the control group. The majority of the studied population reported that they never had bronchial asthma, atopy, and skin allergy i.e. sneezing, nasal discharge, and eye irritation (Table 2).
Table 2. Percentage frequency of questionnaire items.
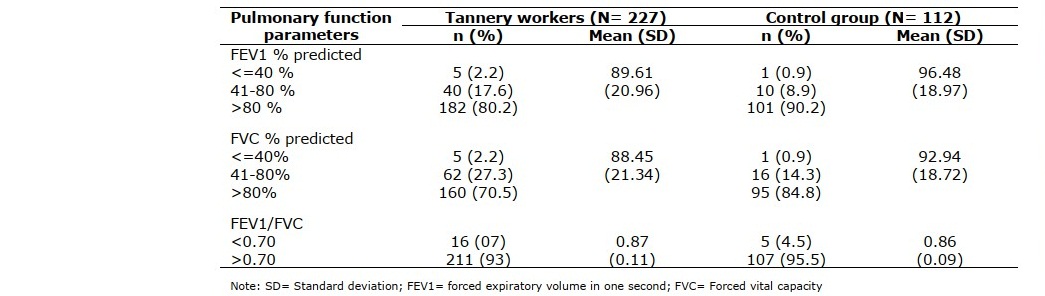
The mean values of pulmonary function parameters in tannery workers were as FEV1 percentage predicted (89.61 ± 20.96), FVC percentage predicted (88.45 ± 21.34), and FEV1/FVC (0.87 ± 0.11). Similarly, in the control group, the obtained mean values were FEV1 percentage predicted (96.48 ± 18.97), FVC percentage predicted (92.94 ± 18.72), and FEV1/FVC (0.86 ± 0.09) (Table 3).
Table 3. Pulmonary function parameters of studied population.
In patterns of respiratory abnormalities, the mixed pattern was dominant in both tannery workers (18.1%) and the control group (7.1%) (Figure 1). While airflow obstruction was reported at the least both in tannery workers (3.1%) and control group (1.8%).
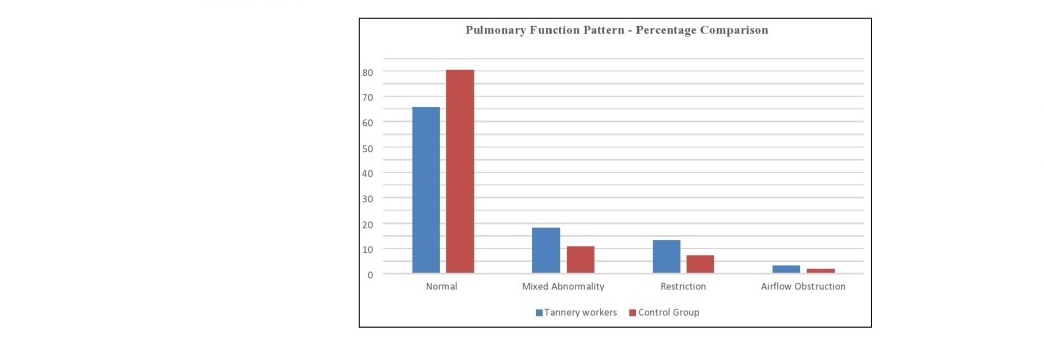
Figure 1. Comparison of Pulmonary function patterns among studied populations.
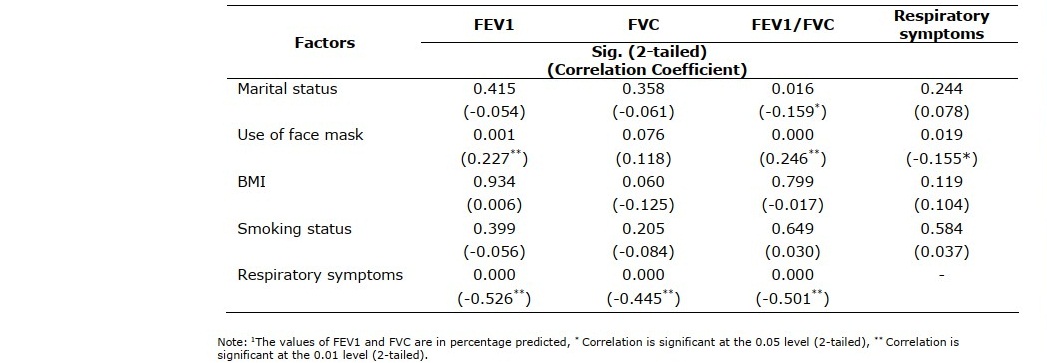
The results of the point biserial correlation showed that respiratory symptoms were negatively correlated with all pulmonary function parameters (FEV1 percentage predicted, FVC percentage predicted, and FEV1/FVC) at the (0.01) significance level. BMI and smoking status were not significantly correlated with the pulmonary function parameters. However, the use of face mask was positively correlated with FEV1 percentage predicted and FEV1/FVC at the (0.01) significance level. While marital status was negatively correlated only with FEV1/FVC at the (0.05) significance level (Table 4).
Table 4. Point-biserial correlation between demographic factors and pulmonary function parameters (N=227).
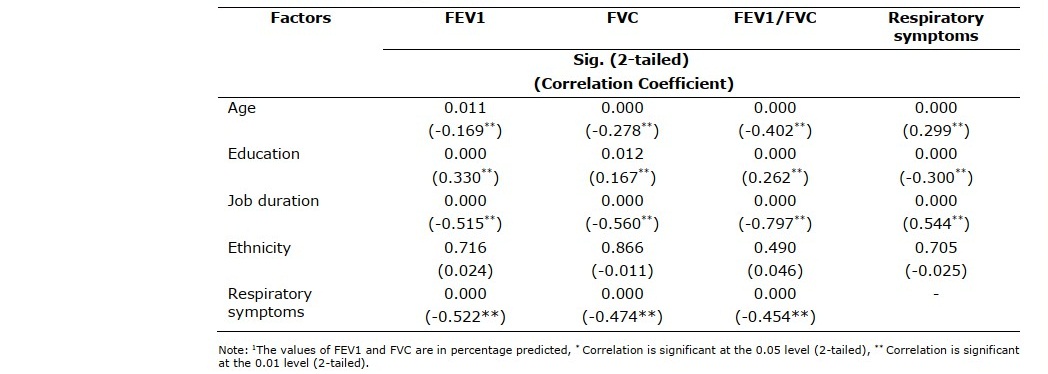
The results obtained through Spearman’s rho correlation showed that age and job duration were negatively correlated with all pulmonary function parameters at the (0.01) and (0.05) significance level. However, education was positively correlated with all pulmonary function parameters at the (0.01) and (0.05) significance level. But ethnicity was not significantly correlated with all pulmonary function parameters (Table 5).
Table 5. Spearman rho correlation between demographic factors and pulmonary function parameters (N=227).
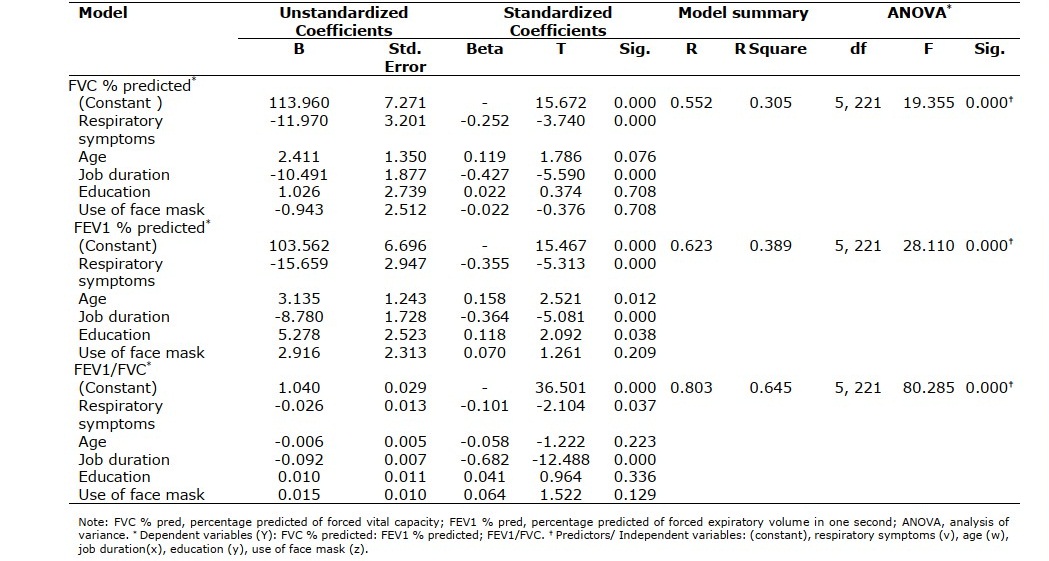
A multiple linear regression was administered to predict FVC percentage predicted, FEV1 percentage predicted, and FEV1/FVC based on respiratory symptoms, age group, duration of job, education and use of face mask (Table 6). In case of FVC percentage predicted a significant regression equation was found (F(5, 221) = 19.35, P < 0.000), with an R2 of 0.305.Assessing only the p-values suggests that the respiratory symptoms and duration of job were equally statistically significant. In fact, age group (P = 0.076), use of face mask (P = 0.708) and education (P = 0.708) did not reach statistical significance in the multiple regression model. The multiple regression model was as follows: Y = 113.96 -11.97 (respiratory symptoms) + 2.41 (age group) - 10.49 (duration of job) + 1.026 (education) -0.943 (use of face mask).
In case of FEV1 percentage predicted a significant regression equation was found (F (5, 221) = 28.11, P < 0.000), with an R2 of 0.389. Assessing only the P-values suggests that the respiratory symptoms, age group, duration of job, education were equally statistically significant. In fact, use of face mask did not reach statistical significance (P = 0.209) in the multiple regression model. The equation of multiple regression model was as follows: Y = 103.562-15.659 (respiratory symptoms) + 3.135 (age group) - 8.780 (duration of job) + 5.278 (education) + 2.916 (use of face mask). Similarly, in case of FEV1/FVC a significant regression equation was found (F (5, 221) = 80.28, P < 0.000), with an R2 of 0.645. Assessing only the p-values suggests that the respiratory symptoms and duration of job are equally statistically significant. In fact, age group (P = 0.223), use of face mask (P = 0.129) and education (P = 0.336) does not reach statistical significance in the multiple regression model. The multiple regression model was as follows: Y = 1.040- 0.026 (respiratory symptoms) - 0.006 (age group) - 0.092 (duration of job) + 0.010 (education) +0.015 (Use of face mask).
Table 6. Multiple Linear regression between pulmonary function parameters, respiratory symptoms and demographic factors (Tannery workers N=227).
DISCUSSION
In the present study, the impaired pulmonary function and respiratory symptoms of wet-blue leather tannery workers were studied. The prevalence of respiratory symptoms recorded through questionnaire in the tannery workers and the control group was 27.8% and 21.4% respectively. The difference might be since the tannery workers were more likely to be exposed to many workplace hazards, including chemical, physical, and biological hazards from raw hides that might aggravate respiratory symptoms (Issever et al., 2007). Similar results were reported in Ethiopia (Dalju et al., 2019) where, prevalence rate among exposed tannery workers was 27.1% and 8.3% in unexposed control group. However, results are higher when compared with 16% (Issever et al., 2007) and 16.7% (Rastogi et al., 2008) investigated among tannery workers. The low prevalence rate could be due to better health of the workers, illness reporting approach and occupational conditions. Moreover, differences in prevalence rate between tannery and non-tannery workers were also reported in Kenya (Were et al., 2014), Egypt (Afify et al., 2013) and India (Chandrasekaran et al., 2014).
In connection with the above, the present result showed a less prevalence of asthma among tannery workers as compared to other researches. A varying prevalence of asthma in workers was reported in different researches. In Istanbul, Turkey, asthma reported among tannery workers were 03% (Issever et al., 2007). In Kanpur, India; it was reported 05% (Thanikaivelan et al., 2004). In Karachi, Pakistan, asthma reported among tannery workers was 10% (Shahzad et al., 2006). However, in present research, bronchial asthma was reported by single tannery worker. The wide difference might be due to different diagnostic criteria, lifestyle, the status of the working environment, and genetic factors.
The tannery workers showed decreased values of pulmonary function parameters (except FEV1/FVC) than the control group. The plausible suggestions for these differences could be the workplace environmental hazards and unused protective equipment by the workers. While in control group such kind of exposure of the workplace was absent. Similar findings were reported among tannery workers in Vellore district, India (Chandrasekaran et al., 2014) and Karachi, Pakistan (Jamal et al., 2017). They concluded that lung function measurements were reduced among tannery workers as compared to the control group.
In tannery workers, impaired pulmonary function recorded as: restriction (13.20%), airflow obstruction (3.10%), and mixed pattern (18.10%) of respiratory abnormalities. However, obstructive pattern among workers was emphasized and frequently reported by other researchers as 14.70% (Rastogi et al., 2008), and 40.27 % (Issever et al., 2007). while in current research it was 3.1 % in tannery workers. The reason for this dissimilarity could be the safest environment in the workplace as well as the better health status of the workers. Similarly, the results of restriction and mixed patterns of the current research were in line with other published data (Chandrasekaran et al., 2014).
In tannery workers, First, age group had shown relationship with FEV1 percentage predicted (r = -0.169, P = 0.011), FVC percentage predicted (r = -0.278, P = 0.000), FEV1/FVC (r = -0.402 P = 0.000), and respiratory symptoms(r = -0.299, P = 0.000). Such statistical significance was also endorsed among tannery workers of Karachi (Jamal et al., 2017) where, age group of > 30 year was associated with respiratory symptoms OR 1.39 (95% CI: 0.33-5.89). Similar findings were corroborated by other researchers among tannery and non-tannery workers (Shahzad et al., 2006; Gao et al., 2018; Gholami et al., 2020). However, discrepancies in results are found when compared with the tannery workers of Ethiopia (age group >35 years OR 1) (Dalju et al., 2019) and Istanbul (P = 0.28) (Ozdilli et al., 2007). It is evident from other researches that the respiratory symptoms increase as the age increases. The performance of the lungs declines with the age factor due to weak muscle strength. Consequently, the lungs become vulnerable to respiratory diseases (Sharma and Goodwin, 2006; Gray et al., 2013).
Second, in the current study education was found to have association with FEV1 percentage predicted (r = 0.330, P = 0.000), FVC percentage predicted (r = 0.167, P = 0.012), FEV1/FVC (r = 0.262, P = 0.000) and respiratory symptoms (r = -0.300, P = 0.000). Similar results were reported among tannery workers of Karachi (Shahzad et al., 2006) where illiterate tannery workers were more likely to have asthma than literate AOR 2.13 (95% CI: 1.17-3.88).
Third, job duration had an association with pulmonary function parameters and respiratory symptoms at the (P = 0.000) significance level. The increased job duration enhances the exposure level at the workplace; ultimately making the lungs prone to impairment. Likewise, the prevalence of respiratory and lung diseases in tannery workers of Karachi (Jamal et al., 2017) reported that job duration of > 4 years is statistically significant with all respiratory symptoms OR 2.89 (95% CI: 0.58-14.30), hence endorse the current results. Such relationship was also proved from other researchers at the same and different workplaces (Issever et al., 2007; Chandrasekaran et al., 2014; Tageldin et al., 2017; Dalju et al., 2019; Yasmeen et al., 2020).
Fourth, the use of face mask was associated with FEV1 percentage predicted (r = 0.227, P = 0.001), FEV1/FVC (r = 0.246, P = 0.000), and respiratory symptoms (r = -0.155, P = 0.019). Different results were reported in different researches. Few results are in line with present research (Offeddua et al., 2016; Dalju et al., 2019). While others reported that there was no association between the use of face mask and respiratory symptoms (Jamal et al., 2017). The contradictory results could be linked with the fact that quality of the face mask is an effective barrier to airborne infections (Sim et al., 2014).
Lastly, BMI, marital status, smoking and ethnicity did not show a significant correlation with respiratory symptoms and pulmonary function parameters. The reasons might be due to ethnic differences that affect the pulmonary functions (Hanizdo et al., 2000; Yap et al., 2001; Fulambarkar et al., 2004; Perez-Padilla et al., 2006). Moreover, variations in age, race and geographical regions may lead possible variations in relationship between BMI and pulmonary functions (Wang et al., 2017). Many researches are in line with our findings. BMI was not associated significantly with the pulmonary function parameters, reported among workers of Iran (Gholami et al., 2020). A study conducted in Istanbul reported that smoking status was not statistically significant for all respiratory symptoms among tannery workers (Issever et al., 2007; Ozdilli et al., 2007).
Furthermore, a multiple linear regression model revealed that respiratory symptoms and duration of job were statistical significant throughout the model for FVC percentage predicted, FEV1 percentage predicted and FEV1/FVC. These results are in partial agreement with the findings (Yasmeen et al., 2020) where, respiratory symptoms after controlling other independent variables, remained significant at the level of 0.000 for FVC percentage predicted and FEV1/FVC. Similar findings in Iran (Gholami et al., 2020) were reported that after controlling smoking, BMI and dust exposure; age and job duration remained statistically significant for both FVC and FEV1/FVC, throughout the linear multiple regression model.
CONCLUSION
In conclusion, the current study suggests that age, education along with the exposure at the workplace may cause increase in impaired pulmonary function, and respiratory symptoms among tannery workers as compared to the control group. To prevent pulmonary function impairments, the periodic medical examinations of the workers, including pulmonary function tests are recommended. Such kind of screening will be helpful in early recognizing respiratory obstructions and consequently the removal of sensitive workers from the workplace before developing chronic respiratory obstruction. We should carry out further research among tannery workers with a large population size from copious tanneries for better understanding related to respiratory-related health problems of the workers.
LIMITATIONS OF THE STUDY
Following limitations may lead to bias results. First, results obtained from the respiratory questionnaire were based on participants’ self-reports. Second, samples were collected from fewer numbers of tanneries and non-response occurred, which may lead to bias. Third, sex influences the pulmonary functions, but female population is missing in current study. Finally, age and educational status is not match-controlled between tannery workers and control group, hence statistical power may reduce.
ACKNOWLEDGMENTS
The authors would like to express special thanks of gratitude in carrying out the statistical analysis by Muhammad Noman Malik.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
REFERENCES
Abbas, M., Nousheen, S., and Fazal, R. 2017. Determination of chromium in nail samples of hide market workers, Lahore. Asian Journal of Agriculture and Biology. 5: 107-112.
Afify, M., Arafa, A., and Maksoud, N.A. 2013. Evaluation of some health hazards among Egyptian leather tannery workers. Journal of Applied Sciences Research. 9: 2959-2964.
Bellamy DD, Booker R, Connellan S, Halpin D. Spirometry in practice [Internet]. London: British Thoracic Society (BTS) COPD Consortium. 2005. [cited 2020 June 1]. Available from: https://www.pennine-gp-training.co.uk/res/spirometry_in_practice%202005.pdf.
Chandrasekaran, V., Dilara, K., and Padmavathi, R. 2014. Pulmonary functions in tannery workers--a cross sectional study. Indian Journal of Physiology and Pharmacology. 58: 206-210.
Dalju, I., Dessie, A., Bogale, L., and Mekonnen, T.H. 2019. Occupational risk factors associated with respiratory symptoms among tannery workers in Mojo town, Southeast Ethiopia, 2018: a comparative cross-sectional study. Multidisciplinary Respiratory Medicine. 14: 1-10.
Faul, F., Erdfelder, E., Lang, A.G., and Buchner, A. 2007. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods. 39: 175-191
Fulambarker, A., Copur, A.S., Javeri, A., Jere, S., and Cohen, M.E. 2004. Reference values for pulmonary function in Asian Indians living in the United States. Chest. 126:1225–1233.
Gao, C., Zhang, X., Wang, D., Wang, Z., Li, J., and Li, Z. 2018. Reference values for lung function screening in 10-to 81-year-old, healthy, never-smoking residents of Southeast China. Medicine. 97: 1-10.
Gholami, A., Tajik, R., Atif, K., Zarei, A.A., Abbaspour, S., Teimori-Boghsani, G., and Attar, M. 2020. Respiratory Symptoms and Diminished Lung Functions Associated with Occupational Dust Exposure Among Iron Ore Mine Workers in Iran. Open Respiratory Medicine Journal. 14: 1-7.
Gray, L.A., Leyland, A.H., Benzeval, M., and Watt, G.C. 2013. Explaining the social patterning of lung function in adulthood at different ages: the roles of childhood precursors, health behaviours and environmental factors. Journal of Epidemiology and Community Health. 67: 905-911.
Hnizdo, E., Churchyard, G., and Dowdeswel, R. 2000. Lung function prediction equations derived from healthy South African gold miners. Occupational and Environmental Medicine. 57: 698–705.
Issever, H., Ozdilli, K., Ozyildirim, B.A., Hapcioglu, B., Ince, N., Ince, H., Isik, E., Akcay, E., Yegenoglu, Y., Erelel, M., and Calak, B. 2007. Respiratory problems in tannery workers in Istanbul. Indoor and Built Environment. 16: 177-183.
Jamal, A., Mehmood, A., Putus, T., Savolainen, H., and Liesivuori, J. 2017. Prevalence of respiratory symptoms, bronchial asthma and obstructive lung disease among tannery workers. Peertechz Journal of Environmental Science and Toxicology. 2: 33-42.
Offeddua, V., Yungb, C.F., Lowc, M.S., and Tamd, C. 2016. Effectiveness of Masks and Respirators Against Respiratory Infections in Healthcare Workers: A Systematic Review and Meta-Analysis. International Journal of Infectious Diseases. 4: 1934- 1942.
Ozdilli, K., Issever, H., Ozyildirim, B.A., Hapcioglu, B., Ince, N., Ince H., Yegenoglu, Y., Susever, S., Erelel, M., Isik, E., and Gedikoglu, G. 2007. Biological hazards in tannery workers. Indoor and Built Environment. 16: 349-357.
Perez-Padilla, R., Valdivia, G., Muino, A., Lopez, M.V., Marquez, M.N., De Oca, M.M., Talamo, C., Lisboa, C., Pertuze, J., Jardim, J.R.B., and Meneze, A.M.B. 2006. Spirometric reference values in 5 large Latin American cities for subjects aged 40 years or over. Archivos de Bronconeumologia. 42: 317–325.
Rasoul, G.M.A., Abou Salem, M.E., Allam, H.K., Kasemy, Z.A., and Younis, F.E. 2017. Health-related disorders on occupational exposure to chromium in a leather tanning factory (Menoufia, Egypt). Menoufia Medical Journal. 30: 92.
Rastogi, S.K., Pandey, A., and Tripathi, S. 2008. Occupational health risks among the workers employed in leather tanneries at Kanpur. Indian Journal of Occupational and Environmental Medicine. 12: 132-5.
Shahzad, K., Akhtar, S., and Mahmud, S. 2006. Prevalence and determinants of asthma in adult male leather tannery workers in Karachi, Pakistan: a cross sectional study. BMC Public Health. 6: 1-7.
Sharma, G., and Goodwin, J. 2006. Effect of aging on respiratory system physiology and immunology. Clinical Interventions in Aging. 1: 253-260.
Sim, S.W., Moey, K.S., Tan, N.C. 2014.The use of facemasks to prevent respiratory infection: a literature review in the context of the Health Belief Model. Singapore Medical Journal. 55: 160-7.
Tageldin, M.A., Gomaa, A.A., and Hegazy, E.A. 2017. Respiratory symptoms and pulmonary function among cotton textile workers at Misr company for spinning and weaving EL-Mahalla, Egypt. Egyptian Journal of Chest Diseases and Tuberculosis. 6: 369-376.
Thanikaivelan, P., Rao, J.R., Nair, B.U., and Ramasami, T. 2004. Progress and recent trends in biotechnological methods for leather processing. Trends in Biotechnology. 22: 181-188.
Townsend, M.C., Lockey, J.E., and Velez, H. 2000. ACOEM position statement. Spirometry in the occupational setting. Journal of occupational and environmental medicine. 42: 228-245.
Wang, S., Sun, X., Hsia, T.C., Lin, X., and Li, M. 2017. The effects of body mass index on spirometry tests among adults in Xi’an, China. Medicine. 96: 1-4.
Were, F.H., Moturi, M.C., and Wafula, G.A. 2014. Chromium exposure and related health effects among tannery workers in Kenya. Journal of Health and Pollution. 4: 25-35.
Yap, W.S., Chan, C.C., Chan, S.P., and Wang, Y.T. 2001. Ethnic differences in anthropometry among adult Singaporean Chinese, Malays and Indians, and their effects on lung volumes. Respiratory Medicine. 95: 297–304.
Yasmeen, R., Ali, Z., Tyrrel, S., and Nasir, Z.A. 2020. Assessment of Respiratory Problems in workers associated with Intensive Poultry Facilities in Pakistan. Safety and Health at Work. 11: 118-124.
OPEN access freely available online
Chiang Mai University Journal of Natural Sciences [ISSN 16851994]
Chiang Mai University, Thailand https://cmuj.cmu.ac.th
Irfan Saleem 1, Zulfiqar Ali1,*, and Ali Hussain2
1 Department of Zoology University of the Punjab, Lahore, Pakistan
2 Department of Wildlife and Ecology University of Veterinary and Animal Sciences, Pattoki, Pakistan
Corresponding author: Zulfiqar Ali, E-mail: zali.zool@pu.edu.pk
Total Article Views
Editor: Korakot Nganvongpanit, Chiang Mai University, Thailand
Article history:
Received: January 1, 2021;
Revised: January 29, 2021;
Accepted: February 3, 2021;
Published online: March 24, 2021