 ISSN: 2822-0838 Online
ISSN: 2822-0838 Online

Effects of Peer-support, Self-management Program on Self-management Behavior and Blood Pressure of Older Adults with Essential Hypertensio
Nichakarn Songthai*, Rarcharneeporn Subgranon,Waree Kangchai and Edwin RosenbergPublished Date : 2019-08-28
DOI : 10.12982/CMUJNS.2014.0042
Journal Issues : Number 3, September - December 2014
ABSTRACT
This study aimed to evaluate the effectiveness of peer-support, selfmanagement program on the self-management behavior and blood pressure of older adults with essential hypertension. A randomized control trial was designed. Eighty-one older adults with hypertension were randomly assigned to two experimental groups and one control group of 27 older adults each. At the fourth and sixteenth week after completing a peer-support, self-management program, participants in the two experimental groups demonstrated statistically significant improvements in self-management behavior and reduced blood pressure that were also significantly different from those of the control group. peer-support, self-management program helped maintain self-management behaviors and reduce blood pressure in older adults with hypertension.
Keywords: Peer-support, Self-management program, Randomized control trials, Self-management behaviors, Blood pressure, Peer-led, Community health workers.
INTRODUCTION
Hypertension is a chronic problem highly prevalent in the elderly. According to the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure (JNC 7), hypertension was observed in a majority of all adults aged 60 and older worldwide (Chobanian et al., 2004). In Thailand, the National Statistics Office (2008) reported lower, but still high rates (31.5%) of hypertension in adults aged 60 and older, in 2007. Furthermore, most elderly patients could not control hypertension (Thanakwang and Kunnasit, 2009), resulting in an increasing risk of fatal complications, such as cardiovascular and cerebrovascular morbidity and mortality (Chobanian et al., 2004) and growing dependence on family and society. As hypertension is long lasting and routinely needs treatment, it often has negative mental, social and economic impacts on elderly patients and their families, as well as imposes an increasing cost burden on the health system.
The goal of hypertension management is to control systolic blood pressure. Reaching this goal requires medication as well as behavior adjustments, such as using hypertension medication, reducing weight, adopting the Dietary Approach to Stop Hypertension (DASH) and reduced sodium diet, decreasing alcohol consumption and smoking, increasing physical activity and relieving stress (Chobanian et al., 2004; Thai Hypertension Society, 2012). Consequently, it is essential to promote such behaviors to patients with hypertension.
Recent literature showed that self-management in patients with hypertension is effective in decreasing both systolic and diastolic blood pressure (Chodosh et al., 2005), increasing self-management capabilities and lowering treatment expenses (Lorig and Holman, 2003). Additionally, Kanfer’s self-management model (Kanfer and Gaelick, 1988) comprising self-monitoring, self-evaluation and self-reinforcement helps increase self-management behaviors and quality-of-life among older persons with hypertension (Kangjai, 2003). Encouraging elderly patients with hypertension to self-manage their condition is an effective method for attaining the behavioral goal and health outcome.
Self-management programs come in several forms, most of which provide knowledge of the illness and problem-solving skills for patients with hypertension. Xue et al. (2008) evaluated a self-management program for hypertension delivered through a voluntary club in the community and found a significant reduction in blood pressure in patients with mild-to-moderate primary hypertension. In previous studies, problem-solving capacity decreases in accordance with increasing age (D’Zurilla, Maydeu-Olivares, and Kant, 1998); implying that developing problem-solving skills may not be appropriate practice for elderly patients with hypertension. The antecedents to self-management derived from the literature were those of information, self-efficacy, support and intention. In fact, it can be argued that elderly individuals need supplementary social support for self-management (Udlis, 2011).
Previous research also showed that self-management support helped to effectively increase self-management behaviors, self-efficiency and the health of patients with persistent ailments (Chan et al., 2010). In addition, peer-support, self-management programs helped elderly patients progressively gain not only health knowledge but also self-management skills (Hayes et al., 2010). Thus, the role of social support in self-management programs led by either peers with hypertension or community health workers (called village health volunteers, or VHVs, in Thailand) is of interest. However, previous studies have not indicated whether VHVs can competently lead self-management programs. In Thailand, some medical professionals believe self-management support led by VHVs should be more effective, while others question whether older adults with hypertension have sufficient ability, owing to their age and experience, to lead self-management support programs. Problematically, VHVs and older adults in Thailand have not received trained before being asked to provide self-management support. Consequently, it is vital to study the effectiveness of peer-support, self-management programs led by trained peers with hypertension (henceforth a peer-led, self-management program), compared with the programs led by trained VHVs on the self-management behaviors and blood pressure of older adults with hypertension (henceforth a VHV-led, self-management program). Accordingly, the objective of this research was to evaluate the effects of peer-support, self-management program on the self-management behaviors and blood pressure of older adults with essential hypertension.
MATERIAL AND METHODS
Study design and sample
This study used a single-blind, randomized control-trial design. In addition, multi-stage, simple random sampling was applied to select 3 out of 15 local healthcare organizations, currently called health-promoting hospitals (HPH). To select participants for the study, seven inclusion criteria were used: 1) age 60 or older; 2) diagnosed with essential hypertension for at least a year; 3) blood pressure of Grade 1 or 2; 4) understood Thai; 5) possessed normal perceptions of date, time, place and person; 6) able to undertake activities by themselves (based on the Mini- Mental State Examination Thai Version 2002: MMSE-Thai 2002); and 7) no persistent disease or disorder that hindered participation in the program (based on Modified Barthel ADL Index: BAI). Subsequently, the authors randomly assigned nine older adults with essential hypertension from each of the three hospitals into one of the two experimental groups, peer-led group and VHV-led group, and one control group, resulting in three groups of 27 subjects each. The peer-led group included 27 older adults with hypertension who attended a program of peer-support, self-management led by six elderly peers with hypertension. The VHV-led group comprised 27 older adults with hypertension who joined the program of peer-support, self-management led by six VHVs. To recruit peer leaders, the authors asked for a group of six volunteers to join each trial group of participants. The first volunteer group consisted of two older adults with hypertension from each of the three hospitals mentioned earlier; the other volunteer group included six VHVs from the same hospitals. Finally, the control group included 27 elderly patients with hypertension who did not participate in either of the aforementioned self-management support programs. Participants were excluded if, during the experiment, they had complications due to hypertension or any other ailment that required hospital admission.
Ethical considerations
Before gathering data, the study sites, proposal and instruments were approved by the Research Ethics Committee of the Faculty of Nursing, Burapha University, Thailand. In addition, the older adults with hypertension received an introductory letter that included the aim of the study, proposed participant activities and appointment schedules. They were also notified of the purpose and processes of the study, confidentiality and anonymity issues, as well as their right to withdraw from the study at any time without repercussions. All willing participants were asked to sign a consent form before data collection.
Intervention
Peer-support, self-management program in this study was run in four phrases: peer-led training, support group, self-management and group visits, as follows.
Phase 1 – Peer-led training. Leader volunteers in the two groups participated in the training of peer-support for older adults with hypertension. The training comprised information support for hypertension management, emotional support using motivation-counseling techniques and appraisal support using self-management skills. The first author ensured the volunteers were well equipped with the necessary knowledge of hypertension management and peer-leadership skills.
Phase 2 – Support group. The volunteer leaders and members of each of the experimental groups exchanged knowledge regarding hypertension and hypertension management behaviors as well as practiced self-management skills.
Phase 3 – Self-management. In week 2 to 6, each of the experimental group members practiced self-management by using hypertension medication, reducing weight, adopting the DASH and reduced-sodium diet, decreasing alcohol consumption and smoking, increasing physical activity, relieving stress and writing a daily journal about home self-management.
Phase 4 – Group visits. From week 3 to 6 in each of the experimental groups, the leaders paid weekly visits to group members to exchange self-management information, emotional support and evaluate their self-management.
For the control group, only treatment was provided. Following data collection, the elderly patients in this group were given the option of attending either the peer-led or VHV-led self-management program, similar to what the patients in the experimental groups experienced.
Instruments and data collection
1. OMRON model HEM-7203 is a tool used to digitally measure blood pressure.
2. A questionnaire with 28 questions related to self-management behaviors of older adults with hypertension was adapted from the treatment adherence questionnaire of patients with hypertension developed by Ma et al. (2012), A panel of five experts assessed content validity. Feedback from the panel was used to revise peer-support, self-management program; session plan; manual of peer support and hypertension self-management; and the daily record of the supporter and older adult for self-monitoring. The internal consistency reliability of the questionnaire was 0.87.
Data were gathered before the experiment and at the fourth and sixteenth week after the experiment in a similar manner by three registered nurses with master’s degrees. The data collectors measured and recorded the blood pressure of the three groups. After the measurements, the data collectors, who were blinded, interviewed the patients regarding their self-management behaviors using the questionnaire of self-management behaviors of older adults with hypertension.
Data analysis
1. The general information was analyzed using descriptive statistics: frequency, percentage, mean values and standard deviations. Chi-square Fisher's exact tests and F-test were used to test differences of groups.
2. The self-management behaviors and blood pressure of the older adults with hypertension at the phases of pre-test, post-test and follow-up were statistically analyzed via repeated measure multivariate analysis of variance (repeated-measure MANOVA). Once the differences in self-management behaviors and blood pressure of the participants between phases were observed, paired Bonferroni was utilized.
3. The differences of self-management behaviors and blood pressure of the older adults with hypertension in peer-led group and in the VHV-led group were analyzed using One-way ANOVA. Once the differences in self-management behaviors and blood pressure of the participants between groups were observed, Bonferroni’s paired comparison was used.
RESULTS
The study yielded three sets of results: characteristics of the sample, assumptions of multivariate analyses and hypothesis tests.
1. Characteristics of the sample of the 81 participants are shown in Table 1.
Table 1. Demographic variables of the peer-led, VHV-led and control groups.
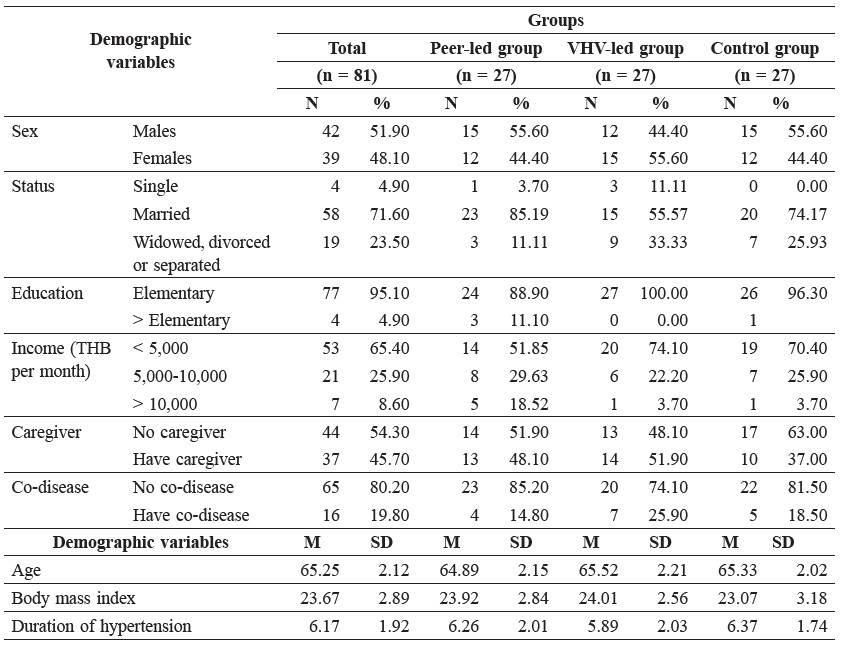
Based on this data, there was no statistically significant difference across the subject groups.
2. Multivariate normal distribution analysis showed normal distributions without outliers. Furthermore, Pearson’s correlation tests showed a statistically significant negative correlation between self-management behaviors and blood pressure without multicollinearity (r = -0.59 and -0.77, respectively; p<0.01). Moreover, the homogeneity of variance-covariance matrices was not statistically significant. Consequently, we concluded that the more self-management behaviors, the lower the blood pressure.
3. Results from hypothesis testing
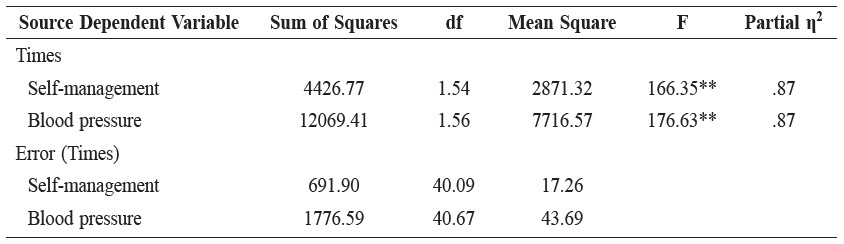
3.1 There was a significant interaction between groups and times on the self-management behaviors and blood pressure (p<.01), as shown in Table 2.
Table 2. Interaction of groups and times on self-management behaviors and blood pressure.

Note: ** p < .01
The results indicated that peer-support, self-management program affected self-management behaviors and blood pressures, both of which changed over the measurement time intervals (Figure 1 and 2)
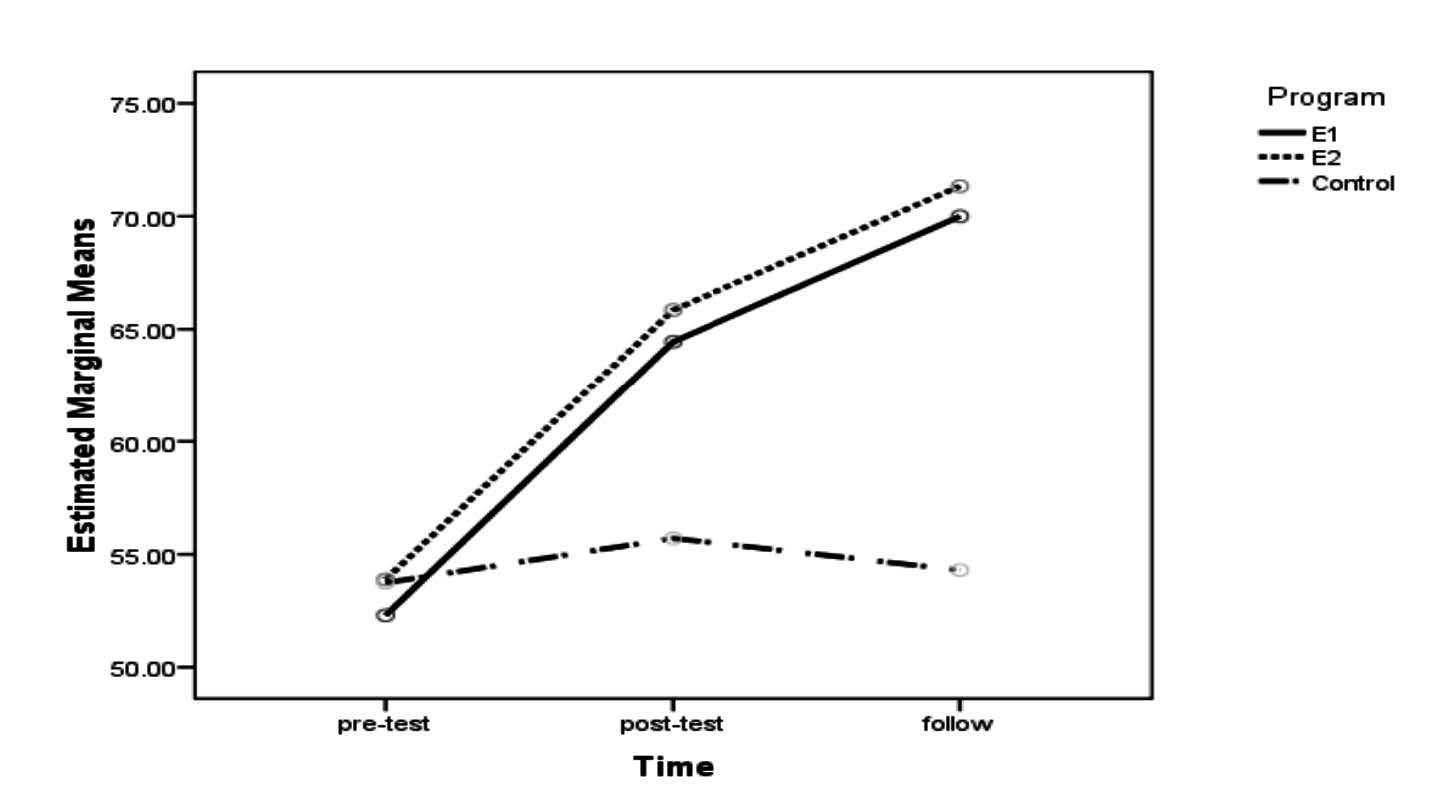
Note: E1 refers to the peer-led group; E2 the VHV-led group.
Figure 1. Change in self-management behaviors of groups at baseline and the 4th and 16th weeks.
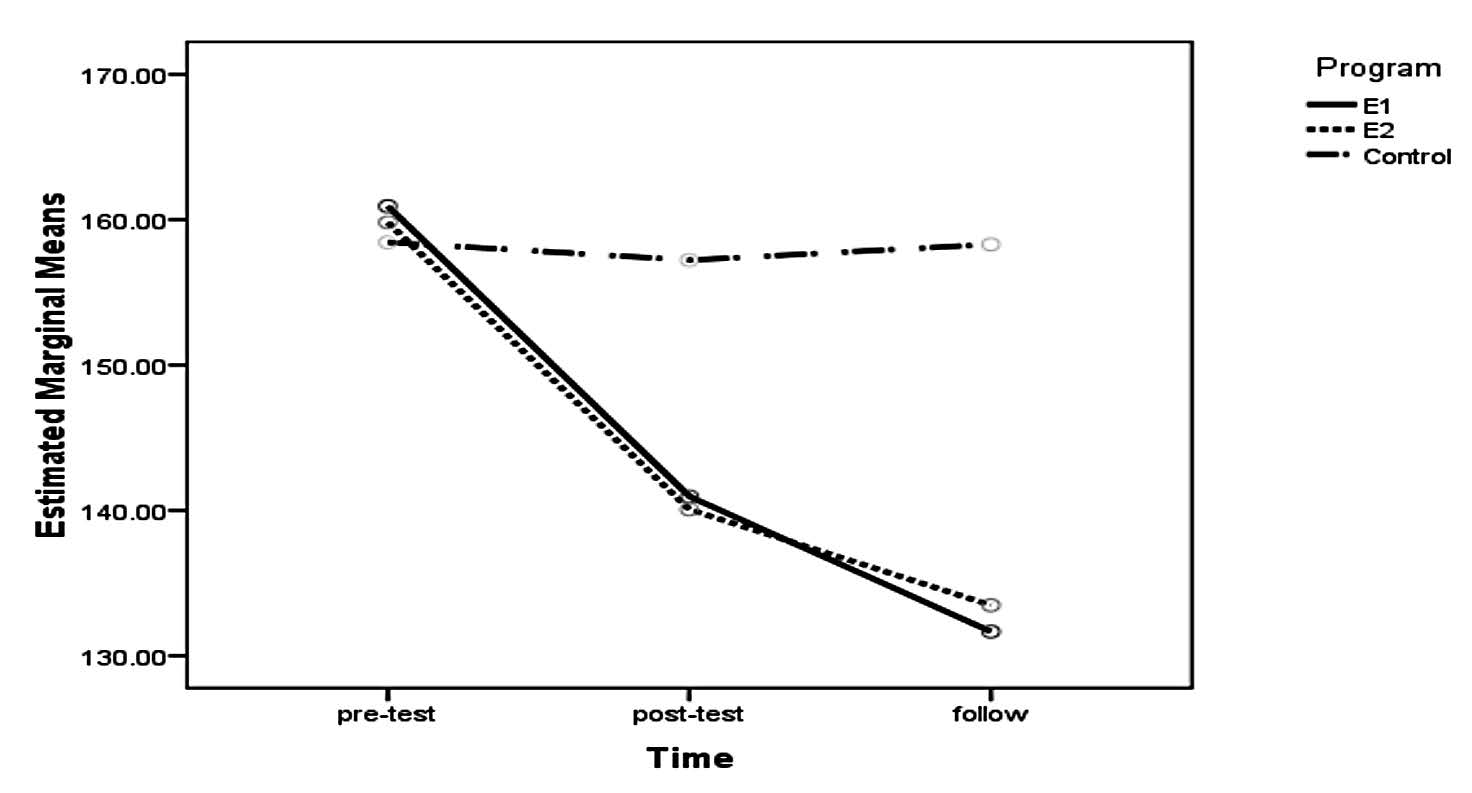
Note: E1 refers to the peer-led group; E2 the VHV-led group.
Figure 2. Change in blood pressures of groups at baseline and the 4th and 16th weeks.
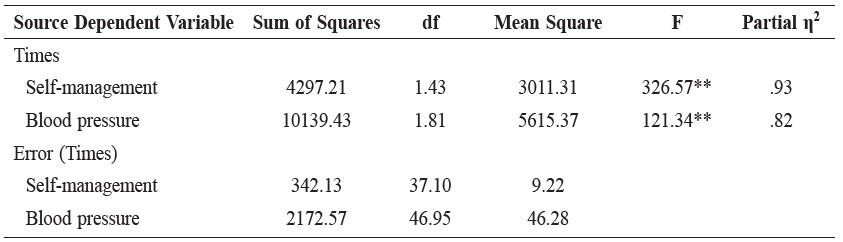
3.2 The self-management behaviors and blood pressure of the older adults with hypertension in the peer-led group significantly improved at the fourth and sixteenth week after the experiment, as shown in Table 2.
Table 2. Simple effects of times on self-management behaviors and blood pressure in the peer-led group.
Note: ** p < .01
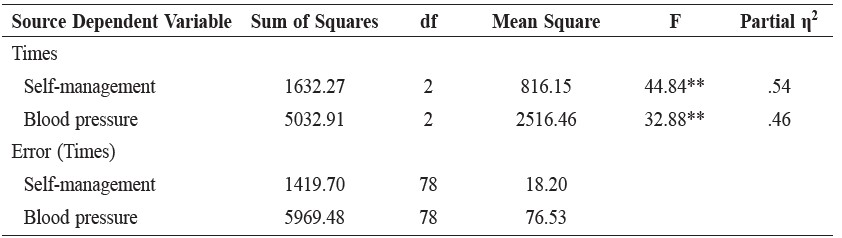
3.3 The self-management behaviors and blood pressure of older adults with hypertension after receiving self-management support in the VHV-led group significantly improved at the fourth and sixteenth week after the experiment, as shown in the table 3.
Table 3. Simple effects of times on self-management behaviors and blood pressures in the VHV-led group.
Note: ** p < .01
As seen in Tables 2 and 3, the self-management behaviors improved and blood pressure decreased in the older adults with hypertension receiving self-management support in both the peer-led group and the VHV-led group.
3.4 In the fourth week after the experiment, the self-management behaviors and blood pressure of the elderly with hypertension who joined the peer-led, self-management program; those of the older adults participating in the VHV-led, self-management program; and those of the patients attending the control group statistically differed at the significance level of 0.01, as shown in Table 4.
Table 4. Simple effects of groups on self-management behaviors and blood pressure at the 4th week after the experiment.
Note: ** p < .01
As significant mean differences of self-management and blood pressure between groups were found, Post hoc test was set at the significance level of 0.01. The results were demonstrated in the table 5.
Table 5. Post hoc in self-management behaviors and blood pressure between the three groups at the fourth 4th and 16th weeks.
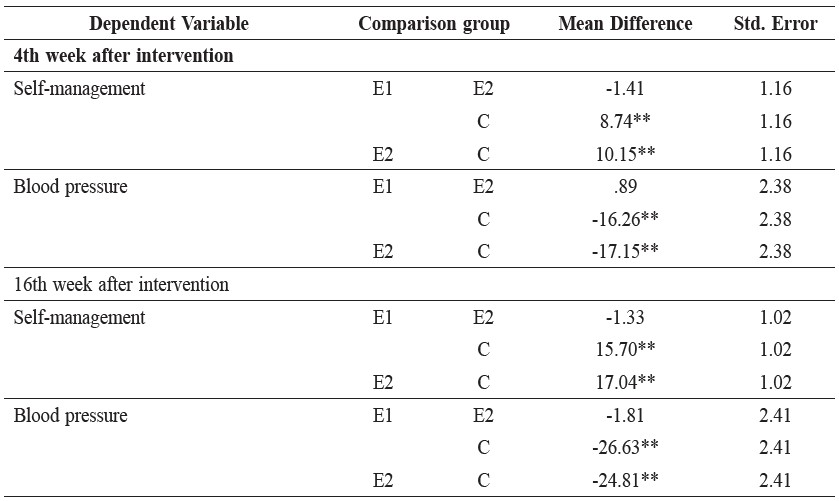
Note: ** p < .01
DISCUSSION
Peer-support, self-management program resulted in increased self-management behaviors and reduced blood pressure in older adults with hypertension. These results are in line with several studies. Mosack et al. (2013) found that peer-support, self-management program could reduce systolic blood pressure in patients with hypertension, with the effect lasting 12 months. Whittle et al. (2014) found that peer-led, self-management support for hypertension significantly decreased blood pressure 12 months after the intervention. Hayes et al. (2010) found that a peer-support, self-management program helped patients with hypertension gain better knowledge and self-management skills.
Since participation in peer-support, self-management program in this study produced a significant reduction in blood pressure and an increase in hypertension management behaviors in older adults with hypertension, this type of program is beneficial for treating older adults with hypertension.
As mentioned earlier, the fundamental belief of Kanfer and Gaelick (1988) stipulates that any individual can better self-manage if motivated, and good behaviors can last only if the individual participates in setting the goal, evaluation and learning processes to effectively self-manage and subsequently retain the hypertension management behaviors.
The significant correlation found in this study between increased self-management behaviors and reduced blood pressure in older adults with hypertension after participating in peer-support, self-management program, either led by peers or by VHVs, is similar to a study in Hong Kong by Chan et al. (2011), who found that peer support for essential self-management knowledge and skill provided to the elderly with chronic diseases, mostly hypertension, was effective. The results in this current study also support the results from a study of community health workers who provided support to people with hypertension (Brownstein et al., 2007). Qualitative research has reported that community health workers can encourage patients to better manage daily behavior, provide social and emotional support, link patients to clinical care and community resources, and provide ongoing support (Kowitt and Emmerling, 2012).
The reduction of blood pressure due to self-management behavior changes in this study corresponds to the concept analysis of Udlis (2011); support is antecedent to self-management itself. Social and emotional support is vital to the success of chronic illness self-management. Furthermore, the behavior of patients with hypertension was also associated with other factors, such as perceptions of the environment and society (Tobin et al., 1986). Therefore, the older adults with hypertension who received informational, emotional and appraisal support from their peers through participation in a self-management program led to changes in general self-management behaviors, i.e., using hypertension medication, weight reduction, adopting a DASH diet and dietary sodium reduction, reducing alcohol consumption and not smoking, and relieving stress. These are compatible with the behavior changes that influence blood pressure reduction (Chobanian et al., 2004; Lorig et al., 2006).
The significant differences between self-management behaviors and blood pressure measured before and after the experiment among the three groups (peer-support, self-management program in the peer-led group; the VHV-led group; and the control) were possibly due to environmental and social factors associated with patients with chronic diseases. Environmental-social factors could help an individual achieve his goal physically and emotionally by stimulating learning and directly affecting the functioning of body organs (Tobin et al., 1986).
Additionally, there was significant improvement in self-management behaviors and decrease of blood pressure, but no significant difference between the older adults with hypertension in the peer-led group and VHV-led group. This result is similar to that found by Tang et al. (2014).
Based on the results in this study, community nurses should use peer-support, self-management programs to support self-management behavior and reduce blood pressure in elderly patients with hypertension. Further studies should compare the effectiveness of peer-support, self-management program in other and wider populations.
ACKNOWLEDGEMENTS
The authors would like to express their deep appreciation to the Office of the Higher Education Commission, Ministry of Education, Thailand, whose grant supported this research.
REFERENCES
Brownstein, N.J., F.M. Chowdhary, S.L. Norris, T. Horskey, L. Jack, X. Zhang, and D. Satterfield. 2007. Effectiveness of community health workers in the care of people with hypertension. American Journal of Preventive Medicine 32(5): 435-447. DOI: 10.1016/j.amepre.2007.01.011
Chan, W.L.S., E. Hui, C. Chan, D. Cheung, S. Wong, R. Wong, S. Li, and J. Woo. 2010. Evaluation of chronic disease self-management program (CDSMP) for older adult in Hong Kong. The Journal of Nutrition, Health and Aging 15(3): 209-214.
Chan, W.L.S., E. Hui, C. Chan, D. Cheung, S. Wong, R. Wong, S. Li, and J. Woo. 2011. Evaluation of chronic disease self-management program (CDSMP) for older adults in Hong Kong. The Journal of Nutrition, Health & Aging 15(3): 209-214. DOI: 10.1007/s12603-010-0257-9
Chobanian, A.V., G.L. Bakris, and H.R. Black. 2004. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Department of Health and Human Services, Boston.
Chodosh, J., S.C. Morton, W. Mojica, M. Maglion, M.J. Suttorp, and L. Hilton. 2005. Meta-analysis: Chronic disease self-management programs for older adults. Annals of Internal Medicine 143(6): 427-438.
D’Zurilla, T.J., A. Maydeu-Olivaresand, G.L. Kant. 1998. Age and gender differences in social problem-solving ability. Personal and Individual Differences 25: 241-252.
Dennis, C.L. 2003. Peer within a health care context: A concept analysis. Nursing Studies 40(3): 321-332.
Hayes, A., J. Morzinski, K. Ertl, C. Wurn, L. Patterson, N. Wike, and J. Whittle. 2010. Preliminary description of the feasibility of using peer leaders
to encourage hypertension self-management. Wisconsin Medical Journal 109(2): 85-90.
Heisler, M. 2006. Building peer support programs to manage chronic disease: Seven model for success. California Health Care Foundation, Oakland. Kanfer, F. H., and L. Gaelick, 1988. Self-management methods. p. 283-245. In F. H. Kanfer, & A. Goldstein (Eds.), Helping people change: A textbook of methods (3rd ed.). Progamon Press, New York.
Kangchai, W. (2003). Efficacy of self-management promotion program for elderly with hypertension. Faculty of Nursing, Burapha University, Thailand.
Kowitt, S., and D. Emmerling. 2012. Balancing standardization and flexibility through a systematic approach: A qualitative study on the activities of village health volunteers in Thailand and the factors that influence their work. Peer for Progress: Peer Support Around the World [Internet]. [cited 2013 May 31]; 1-2. Available from: http://peersforprogress.org/wpcontent/uploads/2012/09/20120925_a_qualitative_study_on_the_activities_of_vhvs. pdf.
Lorig, K. R., and H. Holman. 2003. Self-management education: History, definition, outcomes, and mechanisms. Annals of Behavioral Medicine 26(1): 1-7.
Lorig, K.R., H. Holman, D. Sobel, D. Laurent, V. Gonzalez, and M. Minor. 2006. Living a Healthy Life with Chronic Conditions: Self-management of Heart Disease, Arthritis, Diabetes, Asthma, Bronchitis, Emphysema and Others. Bull Publishing, Colorado.
Ma, C., S. Chen, L. You, Z. Luo, and C. Xing. 2012. Development and psychometric evaluation of the treatment adherence questionnaire for patients with hypertension. Journal of Advance Nursing 68(6): 1402-1413. DOI: 10.1111/j.1365-2648.2011.05835.x
Mosack, K.E., L. Patterson, A.M. Brouwer, A.R. Wendorf, K. Ertl, D. Eastwood, J. Morzinski, K. Fletcher, and J. Whittle. 2013. Evaluation of a peer-led hypertension experiment for veterans: impact on peer leaders. Health Education Research 28(3): 426-436.
Tang, T.S., M. Funnell, B. Sinco, G. Piatt, G. Palmisano, M.S. Spencer, E.C. Kieffer, and M. Heisler. 2014. Comparative effectiveness of peer leaders and community health workers in diabetes self-management support: Results of a randomized controlled trial. Diabetes Care: 1-10. doi: 10.2337/dc13-2161
Thai Hypertension Society. 2012. Guidelines on the Treatment of Hypertension 2012. Thai Hypertension Society, Thailand. National Statistical Office. 2008. Report on the 2007 Survey of the Older Persons in Thailand. National Statistical Office, Thailand.
Thannakwang, K., and P. Kunnasit. 2009. Hypertension unawareness and uncontrolled among adult and elderly people in rural communities, Nan province. Journal of Health Science, 18(1), 10-17.
Tobin, D.L., R.V.C. Reynolds, K.A. Holroyd, and T.L. Creer. 1986. Self-management and social learning theory. p. 29-55. In K. A. Holroyd, and T. L.
Creer (Eds.). Self-management of Chronic Disease: Handbook of Clinical Experiments and Research. Academic Press, London.
Udlis, K. 2011. Self-management in chronic illness: Concept and dimensional analysis. Journal of Nursing and Healthcare of Chronic Illnes 3: 30-139.
Whittle, J., M.M. Schapira, K.E. Flectcher, A. hayes, J. Morzinski, P. Laud, D. Eastwood, K. Ert, L. Patterson, and K.E. Mosack, 2014. A randomized
trial of peer-delivered self-management support for hypertension. American Journal of Hypertension: 1-8. doi:10.1093/ajh/hpu058.
Xue, F., Yao, W., and R. J. Lewin. 2008. A randomised trial of 5 week, manual based, self-management program for hypertension delivered in a cardiac patient club in Shanghai. BioMed Central Cardiovascular Disorders 8(10): 1-11. DOI: 10.1186/1471-2261-8-10
Nichakarn Songthai1*, Rarcharneeporn Subgranon2, Waree Kangchai2 and Edwin Rosenberg3
1 Faculty of Nursing, Burapha University, Chon Buri 20130, Thailand.
2 Faculty of Nursing, Burapha University, Chon Buri 20130, Thailand.
3 Department of Sociology, Appalachian State University, Boone, NC 28608, USA.
*Corresponding author. E-mail: nsongthai@gmail.com
Total Article Views