 ISSN: 2822-0838 Online
ISSN: 2822-0838 Online

Public Knowledge and Awareness of Cardiovascular Diseases and the Expected Role of Community Pharmacists in the Prevention and Management of Cardiovascular Diseases in Penang, Malaysia
Azmi Sarriff*, Arwa M. Amin and Hamza MostafaPublished Date : 2019-08-28
DOI : 10.12982/CMUJNS.2014.0041
Journal Issues : Number 3, September - December 2014
ABSTRACT
This study was carried out to estimate the current knowledge and awareness of cardiovascular diseases (CVDs) and its risk factors among the general public in Penang, Malaysia and to explore public perception of the role of community pharmacists in the prevention and management of CVDs. Four hundred and fifty-six members of the public were given a self-administered, structured questionnaire. The questionnaire was in three languages (English, Malay and Chinese). Those who were illiterate or with prior experience/knowledge in the medical field were excluded from the study. The knowledge and the awareness scores were computed as continuous variables, and then categorized into three levels (poor, moderate and high). The analysis of the results revealed that 46%, 43% and 9% of the respondents had poor, moderate and good knowledge of CVDs and its warning symptoms, respectively. Public awareness of CVD risk factors was better than their knowledge of CVDs and its warning symptoms; in which 37%, 35% and 28% had poor, moderate and good awareness, respectively. Males were more knowledgeable than females. Education level also associated, positively, with knowledge. The majority of respondents gave favorable responses on the role of community pharmacists in identifying and preventing CVD risk factors in the community. This study provides insights into the limited knowledge and awareness of CVDs and its risk factors among the public in Penang, Malaysia and it shows the extended clinical role of community pharmacists in public health and preventing non-communicable diseases. Extensive awareness programs targeting those with limited knowledge are required.
Keywords: Cardiovascular disease, Knowledge, Awareness, Risk factors, Community pharmacist, Malaysia
INTRODUCTION
Cardiovascular diseases (CVDs) are one of the most common causes of non-traumatic death worldwide, affecting men and women at almost equally. In 2008, it was estimated that 17.3 million people died from CVDs, 7.3 millions of them from coronary heart disease and 6.2 million from stroke (Laslett et al., 2012; WHO, 2012). Although deaths due to CVDs are decreasing in high-income countries, they are increasing in low and middle-income countries (WHO, 2012).
As cardiovascular diseases usually develop silently, most CVD patients may not be aware of their disease until an acute event, such as a heart attack or stroke develops (WHO, 2012). Yet, measures can be taken to help in the early prevention of CVDs by controlling the modifiable risk factors, which, if ignored, may lead to cardiovascular events. CVDs' modifiable risk factors include tobacco smoking, alcohol drinking, hypertension, diabetes, hyperlipidemia, obesity and physical inactivity (Pearson et al., 2002; Redberg et al., 2009; Goldstein et al., 2011). The prevalence of these risk factors is increasing worldwide (Daviglus et al., 2012; Laslett et al., 2012; May et al., 2012), as well as in Malaysia (Amplavanar et al., 2010; Cheah et al., 2011). A recent nationwide survey revealed an increase in the prevalence of metabolic syndrome in Malaysia (Mohamud et al., 2011). The lack of awareness discourages people from changing their behavioral risk factors (Al Hamarneh et al., 2011; Muhamad et al., 2012). This increases the demand for public awareness programs on CVDs and risk factors. These awareness programs should be tailored to the public’s existing knowledge. Moreover, easily accessible healthcare professionals, such as community pharmacists, can play a vital role in increasing public awareness.
Studies that estimate the level of public knowledge of disease play a prominent role in the proper design of awareness programs. The findings of these studies can guide the designers of new programs to better focus on areas with limited awareness. Although 80% of global deaths due to CVDs occur in developing countries (Laslett et al., 2012; WHO, 2012), published studies examining the public knowledge of CVDs and its risk factors in developing countries are few. Jafary and colleagues explored the knowledge on coronary heart disease (CHD) among patient attendants (persons accompanying patients) at four tertiary care hospitals in Pakistan (Jafary et al., 2005). The study revealed a gap in participant knowledge on CHD and its risk factors. Saeed and colleagues estimated the knowledge level of modifiable risk factors for coronary atherosclerotic heart disease (CASHD) among emergency room attendants in India (Saeed et al., 2009). The researchers found a lack of knowledge on the modifiable risk factors of CASHD among the participants. In Jordan, Mukattash et al. (2012) determined the level of public knowledge and awareness of CVDs; the majority of participants had poor to moderate knowledge of CVDs. In the same study, the researchers explored the public’s perception of the role of community pharmacists in the prevention and management of CVDs. The majority of participants preferred referring to a community pharmacist for prescribed medications, but preferred referring to other healthcare practitioners for advice on monitoring blood pressure, cholesterol or blood sugar (Mukattash et al., 2012).
Few studies exist on the knowledge and the awareness of CVDs among the public in Malaysia. Arokiasamy (1996) explored the behavior concerning CHD among urban Malaysian workers (managerial/executive and clerical/support personnel) in a group of private business firms in Kuala Lumpur. The majority of respondents were not able to identify high blood pressure and alcohol drinking as CVD risk factors (Arokiasamy, 1996). Moreover, the study found an increase in alcohol consumption compared to tobacco smoking among the responders (Arokiasamy, 1996). In a recent publication, Muhamad et al. (2012) found limited knowledge and practice among female patients in primary care facilities in Kelantan, Malaysia.
Few studies have explored the perception towards the role of community pharmacists in public health and patient education in Malaysia. Hashim et al. (1997) explored the perception of community pharmacists' role among a selected subset of the Malaysian population. The majority of respondents preferred seeking advice from medical doctors on medication use, for minor screening tests and to consult for minor ailments. These finding indicated the public’s lack of understanding of the role of community pharmacists. Hassali et al. (2009) explored the perception of general medical practitioners (GPs) on the role of community pharmacists in a northern state in Malaysia. The study concluded that GPs would support the extension of the role of community pharmacists in activities, such as medication counselling (Hassali et al., 2009). Recently, Sarriff et al. (2012) investigated the views of GPs to the extended role of community pharmacists in the state of Penang, Malaysia. Although, the majority of the responding GPs wanted to involve pharmacists in public health education, they had mixed views on the role of community pharmacists in smoking cessation programs (Sarriff et al., 2012). To date, no published study has determined the level of knowledge and awareness of CVDs and its risk factors among the public in Malaysia, regardless of their gender, health status, ethnicity or career level. Furthermore, no published study has explored public perceptions of the role of community pharmacists in the prevention and management of CVDs in Malaysia.
Besides its strategic location, Penang has the advantage of diverse ethnicity representative of Malaysia: two main majorities, Malay and Chinese; one mainminority, Indians; and other minorities. The aim of the current study is to estimate the level of knowledge and awareness of CVDs and its risk factors among the public in Penang, Malaysia and to explore their expectations on the role of community pharmacists in the prevention and management of CVDs.
MATERIALS AND METHODS
This study was a prospective, cross-sectional study. A self-administered, structured questionnaire was designed after reviewing questionnaires of similar studies (Jafary et al., 2005; Al Hamarneh et al., 2011). The content validity of the questionnaire was appraised by an expert panel, which consisted of an associate professor in clinical pharmacy, a lecturer in clinical pharmacy and three community pharmacists. The questionnaire was initially developed in English, and then translated into Malay and Chinese by native pharmacists of each language. The two translations were back translated to English to ensure accuracy.
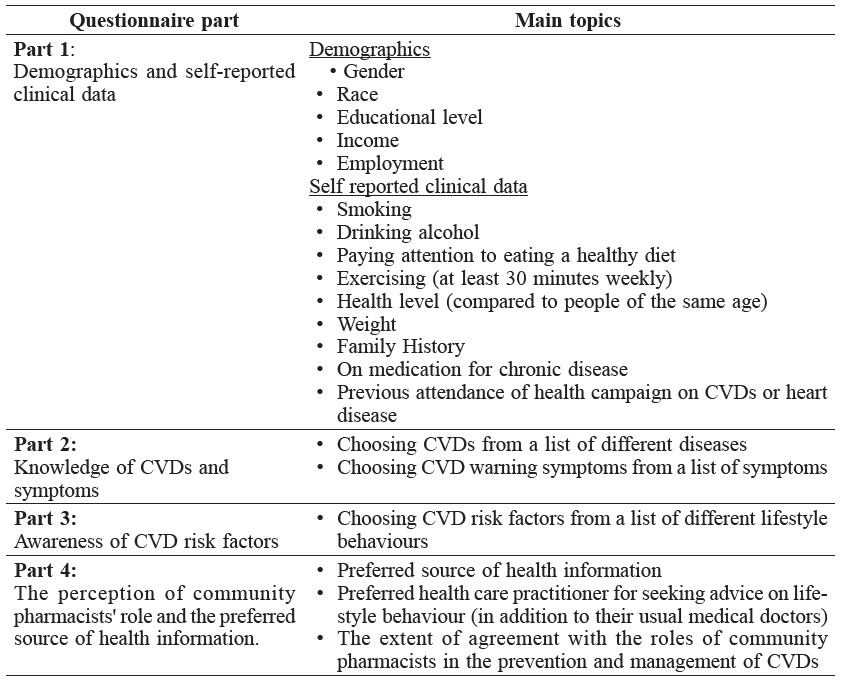
The questionnaire consisted of close-ended questions, structured in four parts: 1) demographic and self-reported clinical data, 2) knowledge of CVDs and its warning symptoms, 3) awareness of CVD risk factors and 4) perception of the community pharmacists' role and the preferred source of health information. Cardiovascular diseases, warning symptoms and risk factors mentioned in the questionnaire were based on those of the World Health Organization (WHO) and the American Heart Association (AHA) (Pearson et al., 2002; WHO, 2010; WHO, 2012). The Joint Ethics Committee of the School of Pharmaceutical Sciences, USM – Hospital Lam Wah Ee on Clinical Studies granted ethical approval to conduct this study. Table 1 shows the parts and main topics of the questionnaire.
Table 1. The parts and main topics of the questionnaire.
After final refinement, the questionnaires were printed in three languages (English, Malay and Chinese) to ensure the achievement of the target sample size within the specified period of data collection. Data was collected over three months (November 2012 to January 2013). The public was approached in different locations in the state of Penang (i.e., residential areas, mosques, shopping centers, shops and bus stops) during all seven days of the week. The researchers interviewed members of the public of both genders who appeared older than 18 years, explained to them the aim of the study and how to fill in the questionnaire. They were then invited to participate in the study. Upon their agreement, they were asked to read and sign the consent form, and then were given the questionnaire to complete. Completing the questionnaire required approximately 10 minutes.
Study Sample
The target sample size was 448, in line with a similar study conducted in Kelantan, Malaysia (Muhamad et al., 2012). The inclusive criteria were male and female members of the public older than 18 years old living in the state of Penang and willing to participate in the study. Those who could not read were excluded. In addition, those with a medical background (i.e., doctors, pharmacists, paramedics and nurses), whether themselves or direct family members, were excluded to eliminate any bias due to professionally-attained knowledge of CVDs and risk factors.
Pilot Study
The questionnaire was pretested for validity and reliability with 20 participants of the public. The pilot study was not included in the research results. Cronbach’s alpha test using SPSS (version 20) software was used to check the consistency of the questionnaire. Cronbach’s alpha of the questionnaire parts was as follows: knowledge part 0.71, awareness part 0.72 and perception on community pharmacists’ role part 0.82.
Scoring of knowledge and awareness
A score of one was assigned for each cardiovascular disease the respondent was able to identify among a list of CVDs and non-CVDs, e.g., lung diseases, and for each symptom the respondent was able to identify as a warning symptom of CVDs. The total score of each participant was computed as a continuous variable. The maximum score for the knowledge part was 13, the minimum was 0. The same scoring was applied to the awareness of CVD risks factor, with a maximum of 14 and minimum of 0. Participants scoring less than 50% of the maximum were considered as having poor knowledge and awareness; 50-70% moderate; and greater than 70% high.
Statistical Analysis
Data were analyzed with SPSS, version 20. Data were cleaned before analyzing demographics and estimating knowledge and awareness levels. Point-biserial correlation and Spearman's correlation tests were used to measure the strength and direction of association between the demographics variables and the knowledge and awareness scores.
RESULTS
Given respondent willingness, 456 questionnaires were collected, more than originally required by the study design. The mean and standard deviation (SD) of the participants' age was 43 and 14.3 years, respectively.
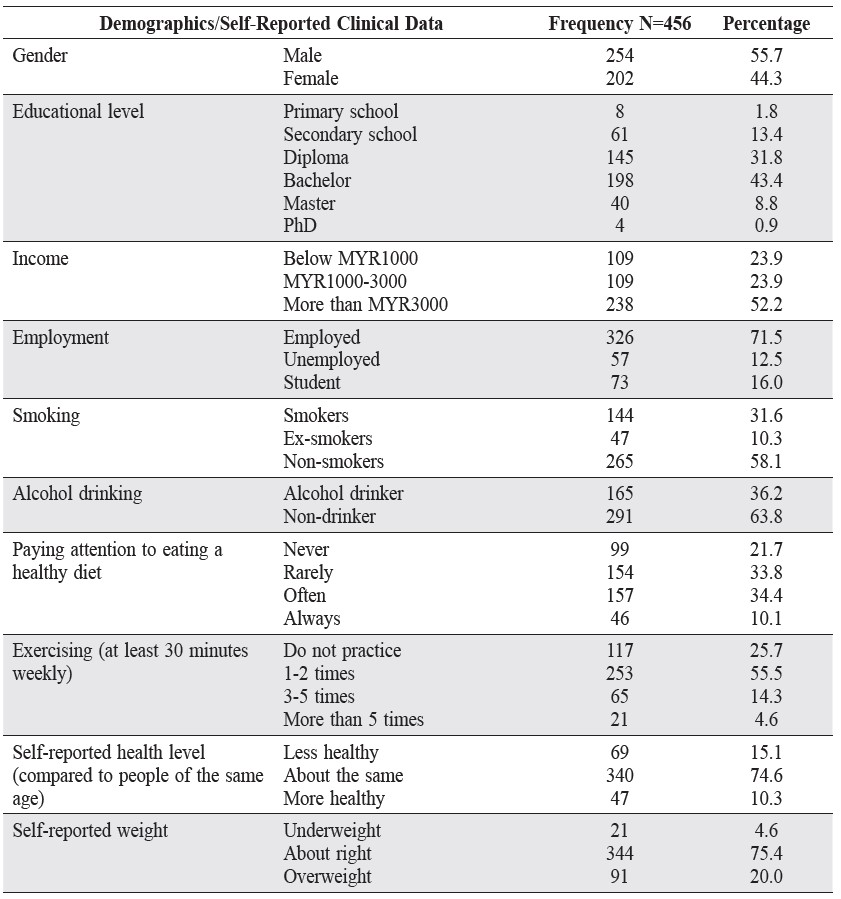
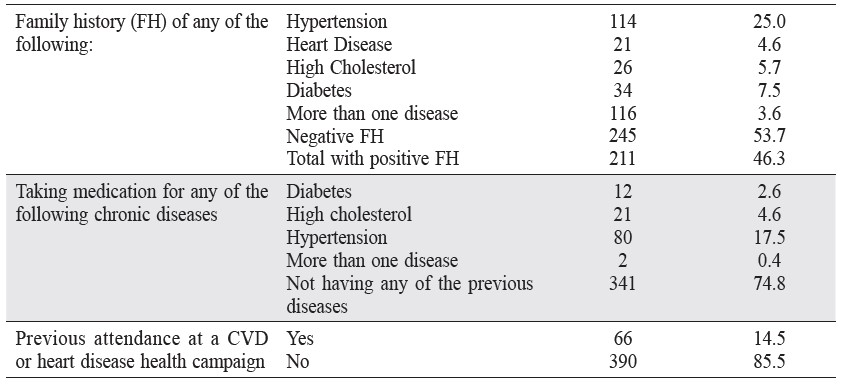
Of the 456 participants, 56% were male. Chinese represented 47% of participants, Malay 39% and Indians 9%. Most of the respondents had tertiary education, the majority was employed and half earned more than MYR 3,000 per month. One third reported smoking; more than one third drank alcohol and over half never or rarely paid attention to eating a healthy diet. Most of the participants reported never having attended a health campaign on heart or cardiovascular disease. Over forty percent reported a family history of one or more cardiovascular-related diseases and/or diabetes, with hypertension the most reported. A quarter of the participants reported having one or more of the following chronic diseases: hypertension, high cholesterol and diabetes. Table 2 shows the demographics and self-reported data of the participants.
Table 2. Demographics and self-reported clinical data.
Most participants showed poor or moderate knowledge of CVDs, with less than 10 percent having high knowledge. The majority of participants showed poor or moderate awareness of CVD risk factors, while almost one third had high awareness. The mean and SD of total knowledge and total awareness scores were (6.5 and 3.3) and (8 and 3.4), respectively. The mean of the total awareness score on CVD risk factors was higher than that of the total knowledge score on CVDs and its warning symptoms. Figure 1 shows levels of knowledge and awareness.
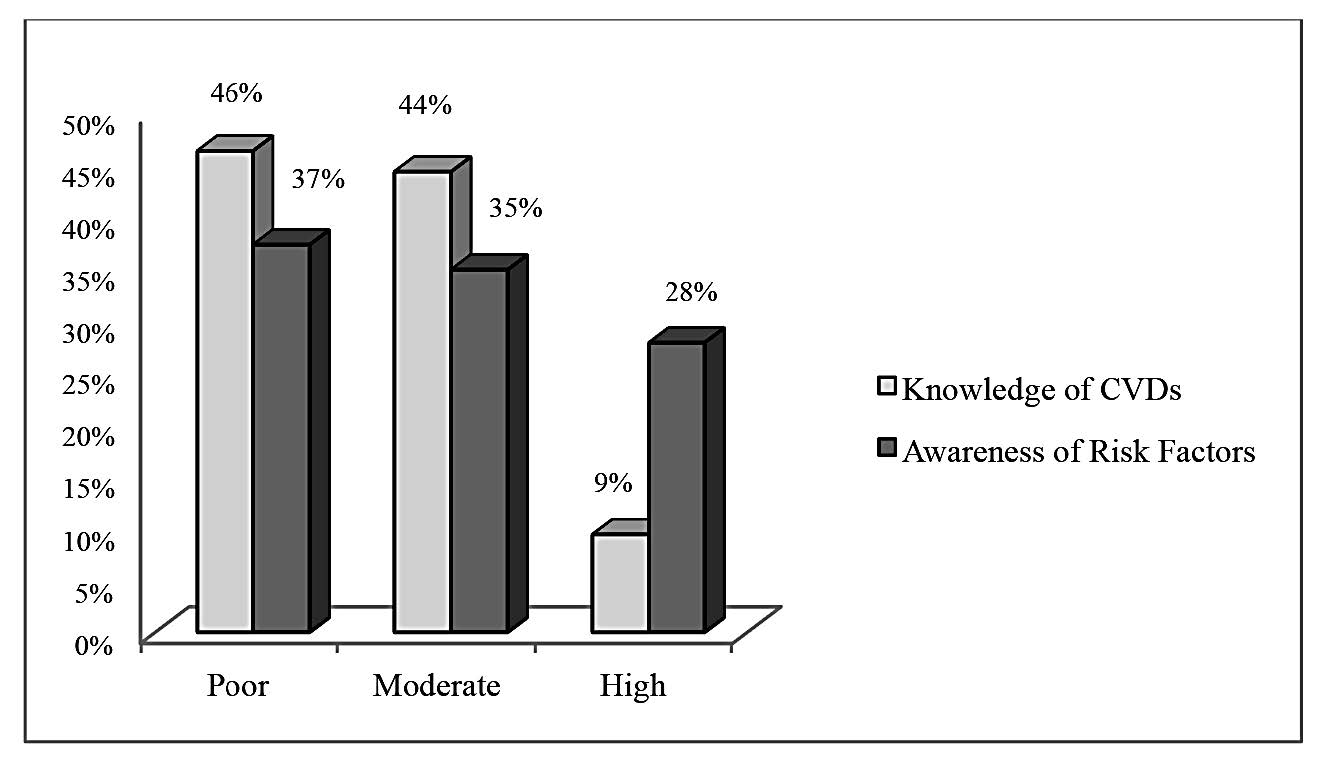
Figure 1. The level (in percent) of Knowledge and Awareness among the study sample.
Of all participants, 22 percent were not able to detect any cardiovascular disease from the four CVDs presented in the knowledge part of the questionnaire (heart disease, peripheral vascular disease, hypertension and coronary heart disease), 20 percent were able to detect one cardiovascular disease and 12 percent were able to detect all four diseases.
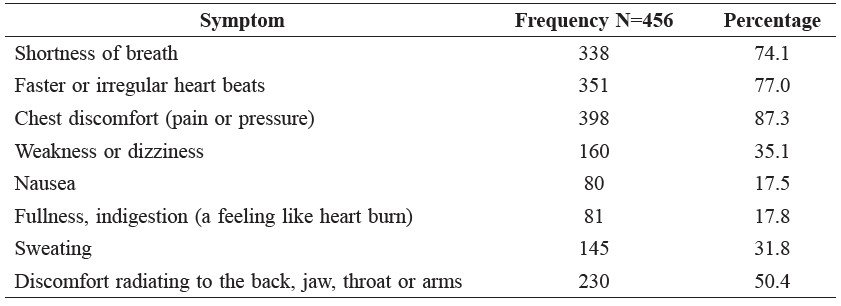
Participants were able to identify the typical warning symptoms of heart attacks or cardiac events (chest pain, shortness of breath, high heart beats) to a high extent compared to atypical symptoms (dizziness, nausea, fullness or heart burn and sweating and discomfort radiating to the back and jaw). Table 3 shows the percent of knowledge of each symptom.
Table 3. Frequency and percentage of participants who detected each CVD symptom.
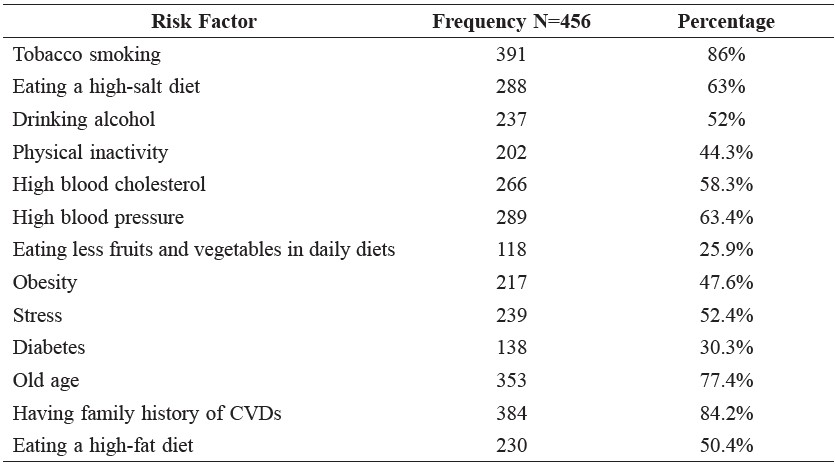
Participants were most aware of tobacco smoking and a family history of CVDs as CVD risk factors. They were least of diabetes and eating less fruits and vegetables in a daily diet. Participants were moderately aware of alcohol drinking, high blood cholesterol, stress, eating a high fat diet and obesity. Table 4 shows the percentage of awareness of each risk factor.
Table 4. Awareness of each risk factor.
Participants most preferred television programs and the Internet as sources for health information. Participants were significantly less interested in radio programs, health magazines and journals, health books and health campaigns. Figure 2 shows respondents preferred health information sources.
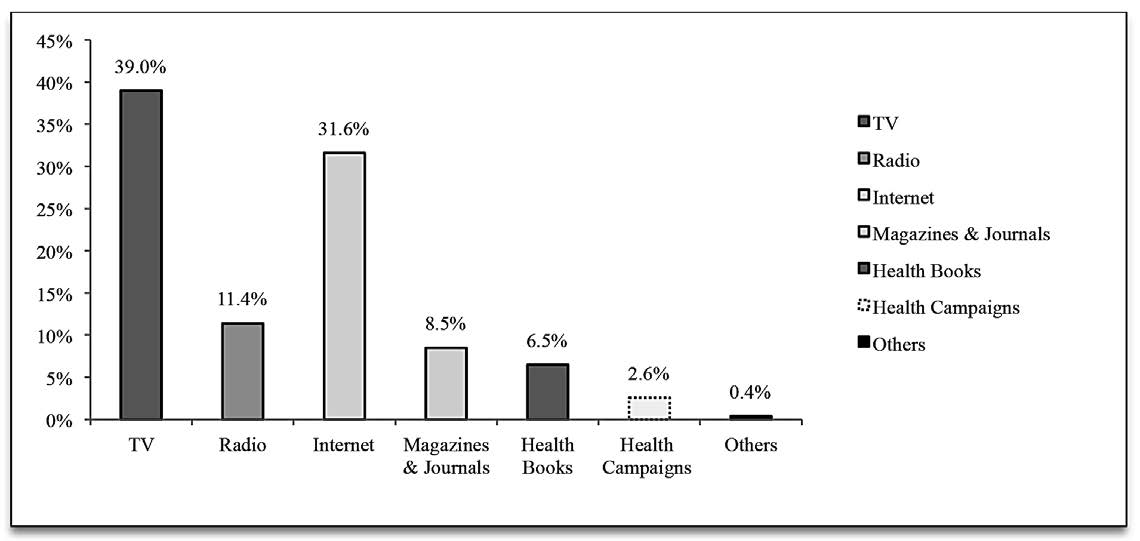
Figure 2. Respondent Preferences for Health Information Sources.
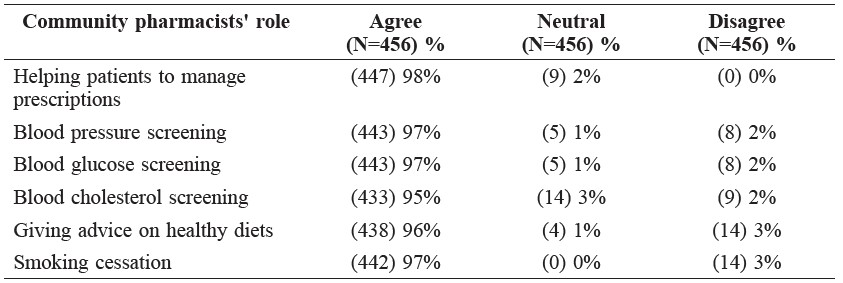
In seeking advice on lifestyle behaviour, in addition to their usual medical doctors, 63% of participants preferred community pharmacists, 17% preferred nurses, 17% preferred dietitians and 3% reported only consulting with their usual medical doctors. When participants were asked to report their level of agreement with the role of community pharmacists in the prevention and management of CVDs, most participants reported they agree that community pharmacists should play a role in helping patients manage prescriptions, screen blood pressure and blood cholesterol and offer advice on healthy diets and quitting smoking (Table 5).
Table 5. Participants' level of agreement with the roles of community pharmacists in the prevention and management of CVDs.
By using point-biserial correlation to measure the strength and direction of association between the dichotomous variables in the demographics, males were found to be more knowledgeable and aware than females. Participants with a family history of one or more CVDs, high cholesterol or diabetes; with hypertension, high cholesterol or diabetes; or who had previously attended a health campaign on heart disease or CVDs were more knowledgeable and aware than those without these traits (Table 6).
Table 6. Point-biserial correlation of dichotomous demographic data and the levels of knowledge and awareness.
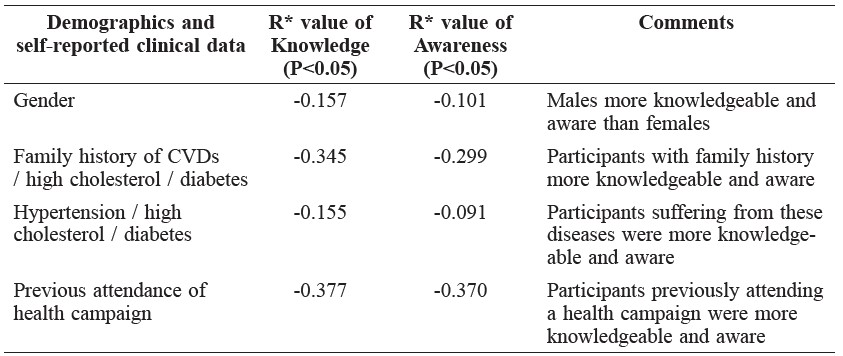
Note: *R: Correlation coefficient.
Spearman's correlation indicated knowledge and awareness were positively associated with increased education levels, increased weekly exercise and healthy diets; and negatively associated with increased weight and age. Personal income and self-reported health level showed no correlation with knowledge and awareness. Table 7 shows the Spearman's correlation between the ranked demographic data and the levels of knowledge and awareness.
Table 7. Spearman correlation between ranked demographic data and the levels of knowledge and awareness.
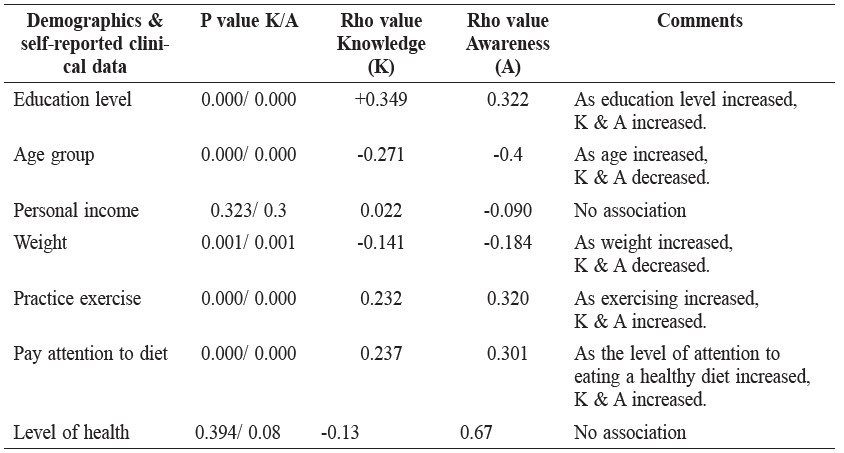
Note: Rho value is Spearman's correlation coefficient.
DISCUSSION
The study found that public knowledge and awareness of CVDs and risk factors was limited in Penang, Malaysia. These results are consistent with other studies conducted in Malaysia and other countries (Arokiasamy, 1996; Jafary et al., 2005; Chow et al., 2008; Saeed et al., 2009; Kandula et al., 2010; Muhamad et al., 2012; Mukattash et al., 2012; Yahya et al., 2012). The majority of respondents reported never having attended a CVD health campaign, which suggests that health campaigns are either not reaching the public or are not being properly promoted. Developing new awareness programs that are attractive, convincing and approachable is required to increase knowledge and awareness.
Respondents were more aware of CVD risk factors than knowledgeable about CVDs and warning symptoms. This implies that current awareness programs are concentrating more on risk factors than warning symptoms. Yet, understanding CVD warning symptoms is critical to patients presenting early and quickly for medical assistance, which results in better outcomes (Sug Yoon et al., 2001; Al Shafaee et al., 2006; Al Hamarneh et al., 2011). Furthermore, the current study found a better awareness of the typical warning symptoms of cardiac events than atypical symptoms. This is similar to other studies (Arokiasamy, 1996; Chow et al., 2008; Muhamad et al., 2012; Mukattash et al., 2012), suggesting that atypical symptoms are not being addressed properly in current awareness programs.
The results showed a higher awareness of smoking than hypertension as a CVD risk factor. This was observed in a similar study in Malaysia (Muhamad et al., 2012). We can infer that the current awareness programs in Malaysia on the harmful effects of smoking are effective. Awareness of hypertension as a CVD risk factor needs more promotion in Malaysia. This contrasts with an American study, where respondents were more likely to identify hypertension than smoking as a CVD risk factor (Lambert et al., 2012). Moreover, the Malaysian respondents showed a lower awareness of obesity, diabetes and high-fat diets as risk factors, compared to other studies conducted in North Ireland, Jordan, India and Pakistan (Jafary et al., 2005; Saeed et al., 2009; Al Hamarneh et al., 2011; Mukattash et al., 2012). All of these findings indicated the importance of tailored awareness programs addressing metabolic syndrome as a CVD risk factor.
The results showed a positive association between knowledge and awareness and the male gender, which might be a warning sign of the lower knowledge and awareness of CVDs among females in the state of Penang, Malaysia. While this is in line with the results of another Malaysian study conducted on females in Kelantan (Muhamad et al., 2012), it contrasts with similar studies in other countries, which showed no association between knowledge of CVDs and gender (Saeed et al., 2009; Al Hamarneh et al., 2011; Mukattash et al., 2012). The consistency of the results in the two Malaysian studies implies weaknesses in reaching females with CVD awareness programs in Malaysia. The positive association between the level of education and the levels of knowledge and awareness in the current study draws attention to the importance of education as a tool to increase public health and quality of life. Moreover, this highlights the need for awareness programs to target people with lower education levels. The results found no association between income and the level of knowledge and awareness. The positive association between family history and knowledge and awareness demonstrated in the current study is probably because awareness increases through seeing the experience of relatives and family members. The negative association between age and the level of knowledge and awareness might be due to the usual attachments of young people to education. The association of paying attention to eating a healthy diet with the level of knowledge and awareness shown in our study is consistent with other studies (Al Hamarneh et al., 2011; Mukattash et al., 2012). This implies that increasing awareness can change behaviors.
As respondents preferred television and the Internet as sources for health information, awareness campaigns should focus on these media.
Our study indicated that the public in Penang has great trust in the role of pharmacists in disease prevention and management, which contrasts with the results of Hashim et al. (2001) more than ten years ago. This may reflect the evolution of the role of pharmacists from medication dispenser to patient-oriented care provider (Wen et al., 2007). The high accessibility of community pharmacists allows them to play a key role in improving public health. The impressive outcome of the community pharmacist interventions in CVDs and other diseases has been proven in several studies (Bouvy et al., 2003; Collins et al., 2011; Martin and Chewning, 2011).
This study has limitations. The use of closed-ended questions in the study questionnaire, where the participant has a list of choices to answer, can raise the chance of guessing, and hence cause bias. As most of the clinical data provided in the demographic part was self-reported, there might be over or under-reporting. This suggests that studies with clinical intervention are required. As illiterates were excluded from the study, studies using oral interviews as a study tool to approach this group are required. Because the random sampling depended on convenience, the representation of Chinese ethnicity in the study was slightly higher than the population. Nevertheless, the population of the study was consistent with the general population of Penang (DOSM, 2012).
REFERENCES
Al Hamarneh, Y.N., G.E. Crealey, and J.C. McElnay. 2011. Coronary heart disease: health knowledge and behaviour. Int J Clin Pharm. 33(1): 111-123 DOI: 10.1007/s11096-010-9467-9
Al Shafaee, M.A., S.S. Ganguly, and A.R. Al Asmi. 2006. Perception of stroke and knowledge of potential risk factors among Omani patients at increased risk for stroke. BMC Neurol. 6: 38. DOI: 10.1186/1471-2377-6-38
Amplavanar, N.T., K. Gurpreet, M.S. Salmiah, and N. Odhayakumar. 2010. Prevalence of cardiovascular disease risk factors among attendees of the Batu 9, Cheras Health Centre, Selangor, Malaysia. Med J Malaysia. 65(3): 173-179.
Arokiasamy, J.T. 1996. Factors and behaviour concerning coronary heart disease in urban Malaysian workers. JUMMEC. 1(1): 33-36.
Bouvy, M.L., E.R. Heerdink, J. Urquhart, D.E. Grobbee, A.W. Hoes and H.G. Leufkens. 2003. Effect of a pharmacist-led intervention on diuretic compliance in heart failure patients: a randomized controlled study. J Card Fail. 9(5): 404-411. DOI: 10.1054/S1071-9164(03)00130-1
Cheah, W.L., P.Y. Lee, Y. Khatijah, and A.W. Rasidah. 2011. A preliminary study on the prevalence of cardiovascular disease risk factors in selected rural communities in Samarahan and Kuching division, Sarawak, Malaysia. Malays J Med Sci. 18(2): 58-65.
Chow, C.-M., J.Y. Chu, J.V. Tu, and G.W. Moe. 2008. Lack of awareness of heart disease and stroke among Chinese Canadians: Results of a pilot study of the Chinese Canadian Cardiovascular Health Project. Canadian Journal of Cardiology. 24(8): 623-628.
Collins, C., B.L. Limone, J.M. Scholle, and C.I. Coleman. 2011. Effect of pharmacist intervention on glycemic control in diabetes. Diabetes Res Clin Pract. 92(2): 145-152. DOI: 10.1016/j.diabres.2010.09.023
Daviglus, M.L., G.A. Talavera, M.L. Aviles-Santa, M. Allison, J. Cai, M.H. Criqui, M. Gellman, A.L. Giachello, N. Gouskova, R.C. Kaplan, and others. 2012. Prevalence of major cardiovascular risk factors and cardiovascular diseases among Hispanic/Latino individuals of diverse backgrounds in the United States. JAMA. 308(17): 1775-1784. DOI: 10.1001/jama.2012.14517
DOSM. 2012. Penang Statistics. Department of Statistics Malaysia.
Goldstein, L.B., C.D. Bushnell, R.J. Adams, L.J. Appel, L.T. Braun, S. Chaturvedi, M.A. Creager, A. Culebras, R.H. Eckel, R.G. Hart, and others. 2011. Guidelines for the Primary Prevention of Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 42(2): 517-584. DOI: 10.1161/STR.0b013e3181fcb238
Hashim, H., A. Mahmud, L.W. Hing, L.P. Yoong, N.M. Yusoff, and T.Y. Bun. 2001. Public Awareness of Community Pharmacy and Pharmacist. Malaysian Journal of Pharmacy. 1(1): 22-28.
Hassali, A., A. Awaisu, A. Shafie, and M. Saeed. 2009. Professional Training and Roles of Community Pharmacists in Malaysia: Views from General Medical Ractitioners. Malaysian Family Physician. 4(2 & 3).
Jafary, F.H., F. Aslam, H. Mahmud, A. Waheed, M. Shakir, A. Afzal, M.A. Qayyum, J. Akram, I.S. Khan, and I. U. Haque. 2005. Cardiovascular health knowledge and behavior in patient attendants at four tertiary care hospitals in Pakistan–a cause for concern. BMC Public Health. 5: 124. DOI: 10.1186/1471-2458-5-124
Kandula, N.R., M.A. Tirodkar, D.S. Lauderdale, N.R. Khurana, G. Makoul, and D. W. Baker. 2010. Knowledge gaps and misconceptions about coronary heart disease among U.S. South Asians. Am J Prev Med. 38(4): 439-442. DOI: 10.1016/j.amepre.2009.12.034
Lambert, C., S. Vinson, F. Shofer, and J. Brice. 2012. The Relationship between Knowledge and Risk for Heart Attack and Stroke. Journal of Stroke and Cerebrovascular Diseases. (0).
Laslett, L.J., P. Alagona, Jr., B.A. Clark, 3rd, J.P. Drozda, Jr., F. Saldivar, S.R. Wilson, C. Poe, and M. Hart. 2012. The worldwide environment of cardiovascular disease: prevalence, diagnosis, therapy, and policy issues: a report from the American College of Cardiology. J Am Coll Cardiol. 60(25 Suppl): S1-49. DOI: 10.1016/j.jacc.2012.11.002
Martin, B.A., and B.A. Chewning. 2011. Evaluating pharmacists’ ability to counsel on tobacco cessation using two standardized patient scenarios. Patient Educ Couns. 83(3): 319-324. DOI: 10.1016/j.pec.2010.12.010
May, A.L., E.V. Kuklina, and P.W. Yoon. 2012. Prevalence of cardiovascular disease risk factors among US adolescents, 1999-2008. Pediatrics. 129(6): 1035-1041. DOI: 10.1542/peds.2011-1082
Mohamud, W.N., A.A. Ismail, A. Sharifuddin, I.S. Ismail, K.I. Musa, K.A. Kadir, N.A. Kamaruddin, N.A. Yaacob, N. Mustafa, O. Ali, and others. 2011. Prevalence of metabolic syndrome and its risk factors in adult Malaysians: results of a nationwide survey. Diabetes Res Clin Pract. 91(2): 239-245. DOI: 10.1016/j.diabres.2010.11.025
Muhamad, R., R. Yahya, and H. M. Yusoff. 2012. Knowledge, Attitude and Practice on Cardiovascular Disease among Women in North-Eastcoast Malaysia IJCRIMPH. Vol. 4(No. 1): 85-98.
Mukattash, T.L., M. Shara, A.S. Jarab, S.I. Al-Azzam, A. Almaaytah, and Y.N. Al Hamarneh. 2012. Public knowledge and awareness of cardiovascular disease and its risk factors: a cross-sectional study of 1000 Jordanians. IJPP. 20(6): 367-376. DOI: 10.1111/j.2042-7174.2012.00208.x
Pearson, T.A., S.N. Blair, S.R. Daniels, R.H. Eckel, J.M. Fair, S.P. Fortmann, B.A. Franklin, L.B. Goldstein, P. Greenland, S.M. Grundy, and others. 2002. AHA Guidelines for Primary Prevention of Cardiovascular Disease and Stroke: 2002 Update: Consensus Panel Guide to Comprehensive Risk Reduction for Adult Patients Without Coronary or Other Atherosclerotic Vascular Diseases. Circulation. 106(3): 388-391. DOI: 10.1161/01.CIR.0000020190.45892.75
Redberg, R.F., E.J. Benjamin, V. Bittner, L.T. Braun, J.D.C. Goff, S. Havas, D. R. Labarthe, M.C. Limacher, D.M. Lloyd-Jones, S. Mora, and others. 2009. ACCF/AHA 2009 Performance Measures for Primary Prevention of Cardiovascular Disease in Adults : A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Performance Measures JACC. 54(14): 1364-1405. DOI: 10.1016/j.jacc.2009.08.005
Saeed, O., V. Gupta, N. Dhawan, L. Streja, J.S. Shin, M. Ku, S. Bhoi, and S. Verma. 2009. Knowledge of modifiable risk factors of Coronary Atherosclerotic Heart Disease (CASHD) among a sample in India. BMC Int Health Hum Rights. 9:2. DOI: 10.1186/1472-698X-9-2
Sarriff, A., N. Nordin, and M. A. A. Hassali. 2012. Extending the roles of community pharmacists: views from general medical practitioners. Med J
Malaysia. 67(6): 577-581.
Sug Yoon, S., R.F. Heller, C. Levi, J. Wiggers, and P. E. Fitzgerald. 2001. Knowledge of stroke risk factors, warning symptoms, and treatment among an Australian urban population. Stroke. 32(8): 1926-1930.
Wen, M.F., S.-J. Lin, Y.-H.K. Yang, Y.-M. Huang, H.-P. Wang, C.-S. Chen, and F.-L. L. Wu. 2007. Effects of a national medication education program in Taiwan to change the public’s perceptions of the roles and functions of pharmacists. Patient Educ Couns. 65(3): 303-310. DOI: 10.1016/j.pec.2006.08.011
WHO. 2010. International Classification of Diseases (ICD-10). World Health Organization.
WHO. 2012. Cardiovascular diseases (CVDs). Volume Fact sheet N°317: Media Center, World Health Organization.
WHO. 2012. Global Atlas on Cardiovascular Diseases Prevention and Control. World Health Organization, World Heart Federation, World Stroke Organization.
Yahya, R., R. Muhamad, and H. M. Yusoff. 2012. Association between Knowledge, Attitude and Practice on Cardiovascular Disease among Women in Kelantan, Malaysia. IJCRIMPH. Vol. 4(No. 8): 1507-1523.
Azmi Sarriff*, Arwa M. Amin and Hamza Mostafa
School of Pharmaceutical Sciences, Universiti Sains Malaysia (USM), 11800 Minden, Penang, Malaysia
*Correspondence: E-mail: azmi@usm.my
Total Article Views