 ISSN: 2822-0838 Online
ISSN: 2822-0838 Online

Validity and Reliability of a Novel Jumping Jacks Test for Estimating Maximal Oxygen Consumption in Healthy Young Adults
Chadaporn Khamjing, Aujima Ngukhiew, Abdulchukkri Kasemsah, Supatcha Konghakote, Pongson Yaicharoen, and Sainatee Pratanaphon*Published Date : December 24, 2024
DOI : https://doi.org/10.12982/NLSC.2025.018
Journal Issues : Number 1, January-March 2025
Abstract Jumping jacks are high-intensity exercises known to improve aerobic fitness and reduce cardiovascular disease risk. However, their effectiveness as a predictor of aerobic fitness has not been well-established. This study aimed to evaluate the validity and reliability of the jumping jacks test (JJT) for estimating aerobic capacity. Twenty-nine healthy adults completed the JJT and the Bruce treadmill protocol to volitional failure, one week apart, in a randomised crossover trial. Maximal oxygen consumption (VO2max) was measured using a gas analyzer. The correlation between VO2max from both tests was assessed using Pearson’s correlation coefficient, and a VO2max prediction equation was developed via stepwise linear regression. Reliability was evaluated in another 16 participants who repeated the JJT twice, one week apart, with intraclass correlation coefficient (ICC) and Bland-Altman plots used for analysis. Our results revealed that VO2max was 34.94 ± 5.02 mL/kg/min for the JJT and 32.15 ± 5.28 mL/kg/min for the Bruce protocol. Significant correlations were found for VO2max (r=0.724, P<0.000) and HRmax (r=0.578, P=0.001), but not for the timed test (r=0.240, P=0.219) or RPE (r=0.324, P=0.093). Two prediction models for VO2max from the JJT were developed: 1) 0.532 × (height, cm) – 54.716, and 2) 0.394 × (height, cm) – 0.310 × (body fat, %) – 25.132, explaining 44.4% and 55.1% of the variance in VO2max, respectively. The repeatability of the JJT for VO2max was excellent (ICC=0.954, P=0.921). In conclusion, the JJT is a valid and reliable method for estimating VO2max in young, healthy adults, offering a practical alternative for assessing aerobic capacity.
Keywords: Jumping jacks, Aerobic testing, Validity, Reliability, Young adults
Citation: Khamjing, C., Ngukhiew, A., Kasemsah, A., Konghakote, S., Yaicharoen, P., and Pratanaphon, S. 2025. Validity and reliability of a novel jumping jacks test for estimating maximal oxygen consumption in healthy young adults. Natural and Life Sciences Communications. 24(1): e2025018.
INTRODUCTION
Cardiorespiratory fitness (CRF) is a key component of health-related fitness, reflecting the efficiency of the cardiopulmonary and skeletal muscle systems in delivering oxygen for physical work. High CRF levels are associated with lower all-cause mortality and reduced risk of hypertension, high cholesterol, and type 2 diabetes (Ross et al., 2016; Kaminsky et al., 2019). CRF is directly measured in the laboratory through maximal oxygen consumption (VO2 max) during cardiopulmonary exercise testing (CPX) with gas exchange analysis, using a cycle ergometer or treadmill. (Ross et al., 2016; Glaab and Taube, 2022). Although CPX is the gold standard being reproducible and safe, it is limited in accessibility due to technical requirements, equipment, and cost. Therefore, indirect methods were developed to estimate CRF using submaximal exercise tests that relate heart rate (HR) response to work rate, and field tests like the 6-minute walk test and various running and walking tests have been developed, as well (Ross et al., 2016). Notably, most of these tests focus on lower limbs movements.
Whole-body exercise like burpees, jumping jacks, and mountain climbers are becoming popular calisthenics training methods. These exercises are effective and safe for improving VO2 max, muscular endurance, and body composition, and can be used by people of different ages and fitness levels (Machado et al., 2019; Menz et al., 2019). Jumping jacks, in particular, are noted for their potential to estimate VO2max due to their simplicity, minimal space requirements, and low cost (Wilke and Mohr, 2020). Boontha et al. (2016a) developed a Jumping Jacks aerobic assessment tool where participants self-paced to reach 70% of their maximal heart rate (HRmax) for 20 minutes, followed by a 30-second acceleration to exhaustion. This method was reported as a safe and vigorous exercise test with excellent repeatability (Intraclass correlation coefficient, ICC = 0.90-0.98) for assessing CRF in young, healthy adults. Participants’ heart rates peaked at 90% HRmax within two minutes, with a rate of perceived exertion (RPE) of 16, and plateaued during the 4th and 5th minutes of recovery (Bootha et al., 2016b).
However, Boontha et al. did not validate the test against a gold standard. To address this limitation, we conducted a pilot study using their CRF protocol and found that the VO2max values obtained were approximately five times lower than those from the Bruce treadmill test, a standard method for assessing VO2max (unpublished data). This discrepancy may have resulted from insufficient exercise intensity. To overcome this issue, our study increased the Jumping Jacks speed based on recommendations from prior research (Town et al., 1980) to ensure adequate intensity. Therefore, this study aimed to evaluate the validity and reliability of the Jumping Jack Test (JJT) for estimating VO2max in young adults.
MATERIAL AND METHODS
Study design and participants
For the validity study, a randomized crossover design was conducted. Participants were randomly assigned to perform either the JJT or the Bruce treadmill test, with each test being separated by a one-week interval. Afterward, the reliability of the JJT was evaluated twice with one week separating each test. Healthy young adults were recruited through social media and flyers were distributed at universities in Chaing Mai Province. Inclusion criteria were as follows: (1) age between 18 and 25 years, (2) body mass index (BMI) between 18 and <25 kg/m², and (3) normal resting heart rate (RHR) and blood pressure (BP), with RHR between 60 to 100 beats per minute, systolic BP less than 120 mmHg, and diastolic BP less than 80 mmHg, as defined in previous research (Liguori et al., 2021; Mason et. al., 2007). Exclusion criteria included any conditions that could affect the study outcomes, such as cardiovascular disease, hypertension, chronic obstructive pulmonary disease, asthma, diabetes mellitus, vertigo, or musculoskeletal injuries of the upper or lower extremities within the last 6 months. Ethical approval was granted by the Institutional Ethical Committee (AMSEC-65FB-009), and informed written consent was obtained from all participants before the study commenced.
Sample size calculation
For validity study, the sample size was calculated based on repeated measures, within factors having a medium effect size (Cohen’s f) of 0.3, a power of 0.8, using G*Power 3.1.9.7. A total sample of 24 participants was required, with an additional 20% attrition rate (n=5) included. Therefore, 29 participants were enrolled in this study. For the reliability study, the sample size was calculated using a hypothesis testing approach (Borg et al, 2022), with a significance level of .05 and a power of 80% to obtain a null Intraclass Correlation Coefficient (ICC) value of 0.95. A total sample of 16 participants was required.
Test protocols
Before testing, participants had their health status verified using a Physical Activity Readiness Questionnaire (PAR-Q+) to confirm their fitness for safe exercise participation (Warburton et al., 2018). Additionally, they were screened by a qualified exercise physiologist. They were instructed to wear comfortable clothes and avoid strenuous exercise, smoking, and alcohol for 24 hours before the test (Glaab and Taube, 2022). The testing protocol included a 5-minute warm-up, the test itself, and a 5-minute cool-down, all conducted at a room temperature of 25°C. The warm-up and cool-down involved a 5-minute dynamic stretching session with triceps stretches, side bends, hip adductor stretches, hamstring stretches, quadriceps stretches, calf stretches, and walking lunges.
Participants were encouraged to exert maximum effort throughout the test, which was supervised by a trained staff. The participants' predicted HRmax was calculated using Nes's formula: 211 - (0.64 × age) (Nes et al., 2013). The exercise tests were terminated if participants reached a HR greater than 85% of their HRmax, a RPE greater than 16, they were unable to continue, or if they exhibited any symptoms that warranted stopping, as indicated by the American College of Sports Medicine guidelines (Liguori et al., 2021).
The Jumping jack test (JJT)
Given the limited data available on jumping jacks, the jump speed in this study was chosen based on rope jumping studies, which found that exercise intensity depends on jumping speed, jumping height, jumping duration, and whether the arms are swung (Quirk et al., 1982; Perantoni et al., 2009; Lyons et al., 2020). Additionally, it was found that rope jumping for five minutes at 125, 135, and 145 skips/min requires a metabolic cost ranging from 11.7 to 12.5 METs (Town et al., 1980). Therefore, a jumping jack cadence of 150 skips/min was chosen to ensure sufficient exercise intensity to induce a submaximal HR within the two-minute test.
The starting position is standing with feet together and arms at the sides. After a 5-minute warm-up, a jumping jack was performed by jumping up and landing with the legs spread wide while lifting arms overhead, then bringing the legs back together and lowering the arms to the sides. Participants were instructed to repeat the jump to achieve 85% of their age-predicted maximum heart rate, using a metronome to stimulate the cadence of 150 skips/min with the jumping height set at 0.5 inch for 2 minutes. A half-inch wooden bar was positioned on the floor as a reference point, and verbal cues were provided to guide participants in matching their jump heights to the set standard. The jumping pace was then increased as fast as possible until exhaustion.
The Bruce treadmill test
A treadmill was used in this study because it has been shown to activate more muscle groups, elicits greater oxygen desaturation, and produces higher levels of peak oxygen uptake (Glaab and Taube 2022). The Bruce protocol consists of walking/running on a treadmill while progressively increasing the speed and incline every three minutes, for six stages. Stage 1, the participant initial started at 1.7 miles per hour (mph) and a 10% gradient, then the velocity increased to 2.5, 3.4, 4.2, 5.0, and 5.5 mph every 3 minutes, simultaneously increased in inclination of 12, 14, 16, 18, and 20.
Data on VO2 max, performance time, heart rate (HR), and maximal heart rate (HRmax) were collected using the Ultima™ CardiO2® gas exchange analysis system (MGC Diagnostics Corporation, MN, USA), and rating of perceived exertion (RPE) was assessed using Borg’s scale (6-20) (Borg, 1970) after both the JJT and the Bruce protocol. Changes in heart rate recovery (HRR) was assessed as the difference between the heart rate peak (HRpeak) at the end of the test and the HR measured at the 1, 2, 3, 4, and 5 minutes of recovery to evaluate physical adaptation to exercise (Cole et al., 1999).
Statistical analysis
Descriptive data was expressed as mean ± SD for continuous normal data distribution and median (interquartile range, IQR) for continuous skewed data. The Shapiro–Wilk test was used to test normality in data distribution. Pearson or Spearman correlation coefficients were used to compare outcome variables — VO2 max, timed test, HRpeak at the end of the test, and RPE —between the JJT and the Bruce protocol. The paired t-test or Wilcoxon signed-rank test, was used to assess differences in these outcome variables between the two aerobic tests. Stepwise linear regression was employed to develop a prediction equation for estimating VO2 max. The intraclass correlation coefficient (ICC) and Bland-Altman plots were used to determine the repeatability and agreement between two trials of the JJT. ICC values of > 0.90 are considered excellent, 0.75 and 0.90 good, 0.50-0.75 moderate, and < 0.50 poor (Koo and Li, 2016). The paired t-test or Wilcoxon signed-rank test was used to assess differences between the two trials of the JJT. All analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 17.0 (SPSS Co., Ltd. Bangkok, Thailand). The significance level was set at P<0.05.
RESULTS
Subject characteristics
The demographic characteristics of the 28 participants (18 male and 10 female) who completed the validity test are summarized in Table 1. One participant withdrew due to illness. One male participant experienced muscle pain in the shoulder and upper arm 1-2 days after the test, which was relieved with cold application and muscle stretching.
Table 1. Demographic data of participants.
|
|
Male (n = 18) |
Female (n = 10) |
Total (n=28) |
Min-Max |
|
Age (yrs) |
20.00 (1.00)a |
20.50 (2.00)a |
20.00 (1.00)a |
18.00 – 22.00 |
|
Body weight (kg.) |
62.19 + 8.02 |
54.30 + 6.85 |
59.38 + 8.43 |
46.00 − 79.00 |
|
Height (cm.) |
171.78 + 4.10 |
161.50 (6)a |
168.54 + 6.29 |
158.00 – 178.00 |
|
Body mass index (kg/m2) |
21.02 + 1.99 |
20.45 + 1.58 |
20.81 + 1.85 |
18.03 − 24.93 |
|
Body fat (%) |
17.15 (4.10)a |
27.06 + 4.80 |
20.58 (5.99)a |
14.00 − 33.50 |
|
Resting heart rate (bpm) |
81.83 + 2.68 |
82.30 + 8.21 |
82.00 + 10.90 |
60.00 – 99.00 |
|
SBP (mmHg) |
124.17 + 2.68 |
117.90 + 7.09 |
124.00 (6.00)a |
105.00 – 128.00 |
|
DBP (mmHg) |
78.33 + 7.28 |
71.70 + 5.42 |
75.96 + 7.33 |
60.00 – 89.00 |
Note: Results are shown as mean ± standard deviation, unless otherwise indicated a median and interquartile range (25th to 75th percentile).
Abbreviations: bpm, beat per minute; cm, centimeter; DBP, diastolic blood pressure; kg, kilogram; m2, square meter; mmHg, millimeters of mercury; SBP, systolic blood pressure; yrs, years.
Validity of the JJT and heart rate recovery
Correlation analysis revealed moderate-to-good correlations between the JJT and the Bruce treadmill test for VO2max (r=0.724, P=0.000) and HRpeak at the end of the test (r=0.422, P=0.025). No-to-fair correlations were found with RPE (r=0.331, P=0.086) and timed test (r=0.240, P=0.219). As shown in Table 2, there were significant differences in VO2max (P<0.001), timed test (P<0.001), HRpeak at the end of the test (P = 0.036), and RPE at the end of the test (P=0.029) between the JJT and the Bruce protocol. As shown in Figure 1, the HRR values after the JJT were comparable to those of the Bruce treadmill test at 1 and 2 minutes post-exercise (all P > 0.05). However, the HRR values for the JJT were significantly higher than those of the Bruce treadmill test at 3, 4, and 5 minutes post-exercise (all P < 0.005).
Table 2. Comparisons in outcomes variables between the Jumping Jacks Test and the Bruce treadmill test.
|
Variables |
Males (n=18) |
Female (n=10) |
Total (Min-Max) |
|
VO2max by the JJT (ml./kg./min) |
37.27 + 4.18 |
30.73 + 3.46 |
34.94 + 5.02* (26.40 – 45.20) |
|
VO2max by the Bruce protocol (ml./kg./min) |
34.14 + 5.03 |
28.55 + 3.65 |
32.15 + 5.28 (23.40 – 41.70) |
|
Timed test for the JJT (min) |
2.36 + 0.78 |
1.76 + 0.87 |
2.15 + 0.85* (0.54 – 4.08) |
|
Timed test for the Bruce protocol (min) |
7.38 + 1.31 |
6.48 + 1.12 |
7.06 + 1.30 (4.26 – 9.41) |
|
HRpeak at the end of the JJT (beats/min) |
156.00 + 12.82
|
153.30 + 10.79
|
155.04 + 12.00* (126.00 – 171.00) |
|
HRpeak at the end of the Bruce protocol (beats/min) |
168.50 (2.25) |
168.00 (3.00)
|
168.00 (1.75)a (138.00 – 172.00) |
|
RPE at the end of the JJT |
13.61 + 2.03 |
14.00 (2.00) |
13.00 (2.00)a, * (9.00 – 17.00) |
|
RPE at the end of the Bruce protocol |
14.00 (3.00) |
16.50 (3.00) |
14.50 (3.00) (12.00 – 18.00) |
Note: Results are shown as mean ± standard deviation, unless otherwise indicated a median and interquartile range (25th to 75th percentile).
* Significant difference with the Bruce protocol (P <0.05)
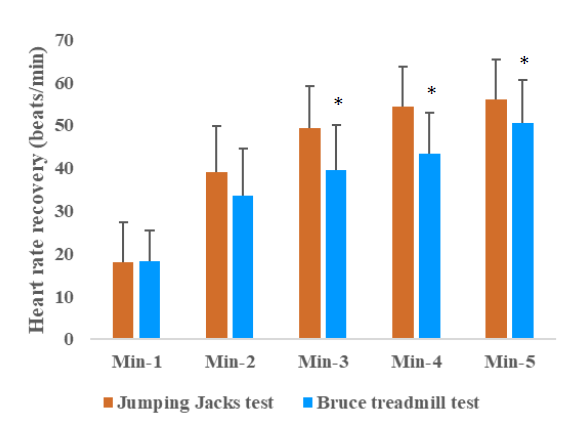
Figure 1. Changes in heart rate recovery (HRR) after 5-minute cessation of the Jumping Jacks Test and the Bruce treadmill test.
Prediction equations for VO2max
All demographic and testing variables with a correlation coefficient of at least 0.20 or −0.20 with VO2max obtained by the JJT were considered in a stepwise multiple linear regression model: age (r=-0.64), body weight (r=0.47), height (r=0.67), PBF (r=−0.60), SBP (r=0.55), DBP (r=0.33), HRpeak at the end of the test (r=0.23), RPE at the end of the test (r=-0.36), and timed test (r=0.33). Due to multicollinearity with VO2max (rs ≥ 0.70), age, PBF, DBP, HRmax, timed test, and RPE were excluded from Model 1, whereas age, DBP, HRmax, timed test, and RPE were removed from Model 2. Sex, BW, SBP were excluded from both models because their inclusion did not significantly improve the model over the existing predictors. The results showed that height alone accounted for 44.4% of the variance in VO2max for the JJT in model 1. In model 2, where both height and PBF were used as predictors, they together explained 55.1% of the variance in VO2 max. These two models are presented in Table 3.
Table 3. Stepwise multiple linear regression analysis with VO2max as the dependent variable.
|
Model |
|
Unstandardized coefficients |
Standardized coefficients |
Collinearity statistic |
||||
|
B |
S.E. |
Beta |
t |
Sig. |
Tolerance |
VIF |
||
|
1 |
Constant |
-54.716 |
19.708 |
|
-2.776 |
0.010 |
|
|
|
|
Height |
0.532 |
0.117 |
0.666 |
4.552 |
<.001 |
1.000 |
1.000 |
|
2 |
Constant |
-25.132 |
21.742 |
|
-1.156 |
0.259 |
|
|
|
|
Height |
0.394 |
0.121 |
0.494 |
3.259 |
0.003 |
0.783 |
1.277 |
|
|
PBF |
-0.310 |
0.127 |
-0.370 |
-2.443 |
0.022 |
0.783 |
1.277 |
Note: Abbreviations: b, slope; SE, standard error; PBF, percent body fat; VIF, variation inflation factor.
Reliability of the JJT
The reliability between the two trials of the JJT was excellent for VO2max (ICC=0.951, P<0.001), moderate for the timed test (ICC=0.682, P=0.001), and poor for HRmax (ICC=-0.080, P=0.620) and RPE at the end of the test (ICC=0.298, P=0.122). There were no differences in VO2max (P=0.921), timed test (P=0.193), HRpeak at the end of the JJT (P=0.530), and PRE at the end of the JJT (P=0.487) between the two trials of the JJT.
Agreement of measurement
The mean VO2max score for the two JJT measurements was 34.87, with a standard error of measurement (SEM) of 0.29 mL/kg/min and a smallest detectable change (SDC) of 0.78 mL/kg/min. The Bland-Altman analysis showed a mean difference (±SD) between the two trials of -1.80 ± 2.65 (95% CI = -7.00 to 3.39; P=0.001). Two participants (12.5%) had results outside the limit of agreement as shown in Figure 2.
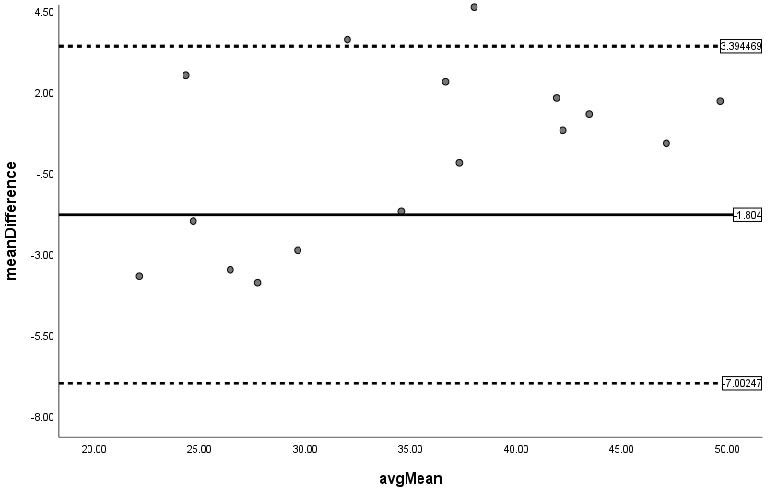
Figure 2. Bland Altman plot with differences in mean of the VO2max between two trials of the Jumping Jacks Test.
DISCUSSION
This study primarily validated the JJT as a reliable and accurate method for estimating VO2max, demonstrating a strong correlation with the Bruce treadmill test. The JJT exhibited excellent reliability, with consistent VO2max measurements across trials, minimal measurement error, and a small SDC relative to the mean VO2max score. The Bland-Altman plot confirmed the test's consistency, indicating narrow limits of agreement between trials. Moreover, the study identified height and percent body fat as significant predictors of VO2max in the context of the JJT. These findings highlight the practical utility of the JJT as a simple, accessible, and cost-effective alternative for VO2max estimation in healthy young adults.
The JJT was performed as a two-minute test followed by exercise to exhaustion at a fixed submaximal work rate, using a metronome set at 150 skips/min. The JJT intensity reached approximately 78% of HRmax, with perceived exertion levels varying between "somewhat hard” for the overall group. For males, this was 79% of HRmax with a "rather hard" rating, and for females, 77% of HRmax with a "hard" rating. In comparison, the Bruce protocol reached 85% of HRmax, with perceived exertion ratings of "hard" for males and "very hard" for females. According to MacIntosh et al. (2021), these intensity levels are classified as vigorous.
The JJT showed lower HRpeak and RPE at the end of the test compared to the Bruce protocol but resulted in higher VO2max, possibly due to the whole-body exercise involved, which may consume more oxygen than the lower-limb-focused Bruce protocol. Additionally, the JJT maintains a consistent, vigorous intensity, whereas the Bruce protocol progressively increases intensity over a longer duration. Despite this, VO2max values from the JJT were lower than reference values reported in other studies, which ranged from 43.3–48.1 ml/kg/min for males (Jones et al., 1985; Wasserman, 2005; van der Steeg, 2021) and 31.8–39.4 ml/kg/min for females (Takken et al., 2019; van der Steeg and Takken, 2021; Wasserman et al., 2005). This discrepancy may be due to differences in genetics, age, body weight, exercise behavior, and testing methods (Ross et al., 2016; Guazzi et al., 2018; Takken et al., 2019; Meyler et al., 2021).
HRR is a key indicator of CRF, reflecting an individual's physical adaptability and the balance between parasympathetic reactivation and sympathetic withdrawal after maximal exercise (Qiu et al., 2017). A faster HRR, marked by a rapid post-exercise HR decrease, indicates better cardiovagal modulation (Facioli et al., 2021; da Fonseca et al., 2024) and depends on rapid parasympathetic activation and progressive sympathetic deactivation (Michael et al., 2017).
Our study found that the reduction in HRR within 5 minutes of JJT cessation followed a similar pattern to findings from previous research (Facioli et al., 2021; da Fonseca et al., 2024), suggesting good cardiovascular autonomic control adaptation among our participants. While no significant changes in HRR were observed during the first two minutes, a marked reduction occurred between 3 to 5 minutes after the JJT compared to the Bruce treadmill test. This suggests that the JJT may elicit a delayed but robust parasympathetic reactivation, possibly due to the dynamic, whole-body movements it involves. The greater HRR reduction during this period may reflect enhanced vagal tone recovery following vigorous, rhythmic exercise, contrasting with the a submaximal graded exercise mode of the Bruce test. However, the exact mechanisms underlying this distinct HRR pattern remain unclear, warranting further investigation.
In this study, prediction equations for VO2max based on height and/or percent body fat showed moderate accuracy (R² = 0.44 - 0.55, with standard errors of estimate (SEEs) between 3.50 and 3.82 mL/kg/min). This results are consistently with findings of a previous study that reported a negative correlation between body fat and VO2max (Bhattachar et al., 2023), while height showed inconsistent results. Notably, the study that found no correlation between height and CRF used a 12-minute run and walk test (Bhowmik, 2024), whereas another study (Siahkouhian, 2009) revealed that tall young men had higher VO2max values in the Queen’s step and maximal treadmill tests compared to shorter individuals. Moreover, both groups exhibited higher VO2max values in the Queen’s step test compared to the treadmill test, consistent with this study’s findings of higher VO2max values in the JJT than the treadmill test. This suggests that the influence of height on VO₂max may depend on the complexity and biomechanical demands of the exercise methodology. Dynamic movements, such as jumping jacks or step tests, require greater control of body segments, potentially favoring taller individuals with longer limbs, while simpler, planar tests like treadmill running may minimize the effect of height. Further investigation is needed to clarify how exercise modality impacts the relationship between height and cardiorespiratory fitness.
Some variables were excluded from the models due to multicollinearity and their minimal contribution to enhancing the prediction model. Furthermore, the small sample size likely contributed to lower R² values, as noted by Dhiman et al. (2023). These limitations may have reduced the overall predictive power of the model, underscoring the importance of conducting studies with larger sample sizes to improve prediction accuracy and ensure more robust conclusions.
The JJT demonstrated moderate repeatability for the timed test, while HRpeak and RPE at the end of the test showed poor reliability. Nonetheless, the lack of significant differences in these parameters between trials suggests that the JJT generally provides consistent results, even if some measures exhibit variability. The study highlights the JJT's potential as a practical tool for self-monitoring cardiovascular fitness in young adults, particularly in settings with limited time, space, or access to specialized equipment such as treadmills or gas analyzers. It may also support lifestyle interventions and progress tracking over time.
The strengths of this study include conducting both aerobic tests at the same time of day and employing consistent protocols, which enhances the reliability of the results. Additionally, the strong correlation and excellent test-retest reliability of the JJT underscore its validity as a fitness assessment tool. However, the JJT has some limitations. Due to its brief and intense nature at a speed of 150 skips/min, only 83.33% (15 out of 18) of males and 50.00% (5 out of 10) of females completed the test. This suggests that the JJT, originally developed for healthy individuals, may not be suitable for all participants, particularly females. Factors such as gender, body stature, and baseline CRF may influence the results. Additionally, the small sample size limits the generalizability of the findings (Riley et al., 2020). Future research should focus on adapting the test for broader applicability and include larger sample sizes.
CONCLUSION
The JJT demonstrated strong reliability and validity in estimating VO2max compared to the Bruce treadmill test, indicating its potential as a practical alternative tool for assessing cardiovascular fitness in young, healthy adults. Its simplicity and ease of implementation may make it a useful option for self-monitoring cardiovascular fitness. Further research is needed to refine the test for individuals with varying physical activity levels and settings.
ACKNOWLEDGEMENTS
We would like to extend our gratitude to the participants for their involvement and valuable contributions to this study. We also thank the Department of Physical Therapy, Faculty of Associated Medical Sciences, Chiang Mai University for providing the gas exchange analysis system and anthropometric instruments.
AUTHOR CONTRIBUTIONS
Chadaporn Khamjing and Sainatee Pratanaphon: concept and study design, analyzed data, wrote, reviewed, and edited the manuscript. Aujima Ngukhiew, Abdulchukkri Kasemsah, Supatcha Konghakote and Pongson Yaicharoen: concept data, reviewed, and edited the manuscript. All authors have read and approved of the final manuscript.
CONFLICT OF INTEREST
The authors declare that they hold no competing interests.
REFERENCES
Bhattachar, S., Chawla, A., Sikri, G., and Patrikar, S. 2023. Body fat content correlates with maximum aerobic capacity in healthy sedentary Indian males. Medical Journal Armed Forces India. 79: 93-100. https://doi.org/10.1016/j.mjafi. 2021.09.004.
Bhowmik, A. 2024. Body height impact on cardiorespiratory fitness among physically active adults. International Journal of Sport, Exercise and Health Research 8(1): 11-14. https://doi.org/10.31254/sportmed.8103.
Boontha, K., Pirunsan, U., Khamwong, P., and Pratanaphon, S. 2016a. Reliability of heart rate maximizer test using jumping jack in assessing cardiovascular fitness. Journal of Associated Medical Sciences. 49(3): 344-354. https://doi.org/10.14456/jams.2016.34
Bootha, K., Pirunsan, U., and Khamwong, P. 2016b. Cardiovascular response and energy expenditure of a novel heart rate maximizer test in healthy volunteer. Journal of Associated Medical Sciences. 49(2): 263-275. https://doi.org/10.14456/ jams.2016.17
Borg, D. N., Bach, A. J. E., O’Brien, J. L., and Saiani, K. L. 2022. Calculating sample size of reliability studies. American Academy of Physical Medicine and Rehabilitation. 14: 1018-1025. https://doi.org/10.1002/pmrj.12850.
Borg, G. 1970. Perceived exertion as an indicator of somatic stress. Scandinavian Journal of Rehabilitation Medicine. 2(2): 92-98.
Cole, C. R., Blackstone, E.H., Pashkow, F. J., Snader, C. E., and Lauer, M. S. 1999. Heart–rate recovery immediately after exercise as a predictor of mortality. New England Journal of Medicine. 341(8): 1351-1357. https://doi.org/10.1056/ NEJM1999 10283411804.
da Fonseca, R. X., da Cruz, C. J. G., von Koenig Soares, E. M. K., Garcia, G. L., Porto, L. G. G., and Molina, G. E. 2024. Post‑exercise heart rate recovery and its speed are associated with resting‑reactivity cardiovagal modulation in healthy women. Scientific Reports. 14(1): 5526. https://doi.org/10.1038/s41598-024-51842-w.
Dhiman, P., Ma, J., Qi, C., Bullock, G., Sergeant, J. C., Riley, R. D., and Collins, G. S. 2023. Sample size requirements are not being considered in studies developing prediction models for binary outcomes: A systematic review. BMC Medical Research Methodology. 23: 188. https://doi.org/10.1186/s12874-023-02008-1.
Facioli, T. P., Philbois, S. V., Gastaldi, A. C., Almeida D. S., Maida, K. D., Rodrigues, J. A. L., Sánchez‑Delgado, J. C., and Souza, H. C. D. 2021. Study of heart rate recovery and cardiovascular autonomic modulation in healthy participants after submaximal exercise Scientific Reports. 11: 3620. https://doi.org/10.1038/ s41598-021-83071-w.
Glaab, T. and Taube, C. 2022. Practical guide to cardiopulmonary exercise testing in adults. Respiratory Research. 23(1): 9. https://doi.org/10.1186/s12931-021-01895-6.
Guazzi, M., Arena, R., Halle, M., Piepoli, M. F., Myers, J., and Lavie, C. J. 2018. 2016 focused update: Clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations. European Heart Journal. 39: 1144-1161. https://doi.org/10.1093/eurheartj/ehw180.
Jones, N. L., Makrides, L., Hitchcock, C., Chypchar, T., and McCartney, N. 1985. Normal standards for an incremental progressive cycle ergometer test. American Review of Respiratory Disease. 131: 700-708. https://doi.org/10.1164/arrd.1985.131.5.700.
Kaminsky, L. A., Arena, R., Ellingsen, Ø., Harber, M. P., Myers, J., Ozemek, C., and Ross, R. 2019. Cardiorespiratory fitness and cardiovascular disease - the past, present, and future. Progress in Cardiovascular Diseases. 62(2): 86-93. https://doi.org/10.1016/j.pcad.2019.01.002.
Koo, T. K. and Li, M. Y. 2016. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. Journal of Chiropractic Medicine. 15(2): 155-163. https://doi.org/10.1016/j.jcm.2016.02.012
Liguori, G., Feito, Y. and Fountaine, C.J. and Roy, B. 2021. ACSM’s guidelines for exercise testing and prescription. 11th ed. Wolters Kluwer, Philadelphia.
Lyons, T. S., Navalta, J. W., Stone, W. J., Arnett, S. W., Schafer, M. A., and Igaune, L. 2020. Evaluation of repetitive jumping intensity on the digi-jump machine. International Journal of Exercise Science. 13(2): 818-825.
Machado, A. F., Baker, J. S., Figueira Junior, A. J., and Bocalini, D. S. 2019. High‐intensity interval training using whole‐body exercises: training recommendations and methodological overview. Clinical Physiology and Functional Imaging. 39(6): 378-383.
MacIntosh, B. R., Murias, J. M., Keir, D. A., and Weir, J. M. 2021. What is moderate to vigorous exercise intensity? Frontiers in Physiology. 12: 682233. https://doi.org/ 10.3389/fphys.2021.682233.
Mason, J. W., Ramseth, D.J., Chanter, D.O., Moon, T.E., Goodman, D.B., and Mendzelevski, B. 2007. Electrocardiographic reference ranges derived from 79,743 ambulatory subjects. Journal of Electrocardiology. 40(3): 228–234. https://doi.org/10.1016/j.jelectrocard.2006.09.003.
Menz, V., Marterer, N., Amin, S. B., Faulhaber, M., Hansen, A. B., and Lawley, J. S. 2019. Functional vs. running low-volume high-intensity interval training: Effects on VO2max and muscular endurance. Journal of Sports Science and Medicine. 18(3): 497-504.
Meyler, S., Bottoms, L., and Muniz-Pumares, D. 2021. Biological andmethodological factors affecting V̇O2max response variability to endurance training and the influence of exercise intensity prescription. Experimental Physiology. 106:1410–1424. https://doi.org/10.1113/EP089565.
Michael, S., Graham, K. S., and Davis, G. M. 2017. Cardiac autonomic responses during exercise and post-exercise recovery using heart rate variability and systolic time intervals—a review. Frontiers in Physiology. 8: 301. https://doi.org/10. 3389/fphys.2017.00301.
Nes, B. M., Janszky, I., Wisløff, U., Støylen, A., and Karlsen, T. 2013. Age-predicted maximal heart rate in healthy subjects: The HUNT Fitness Study. Scandinavian Journal of Medicine & Science in Sports. 23(6): 697-704. https://doi.org/10.1111/j.1600-0838.2012.01445.x
Perantoni, C. B., Deresz, C. S., Lauria, A. A., Lima, J. R. P., and Novaes, J. S. 2009. Analysis of intensity during a session of jump training. Fitness & Performance Journal. 8(4): 286-290. https://doi.org/10.3900/FPJ.8.4.286.E.
Qiu, S., Cai, X., Sun, Z., Li, L., Zuegel, M., Steinacker, J. M., and Schumann U. 2017. Heart rate recovery and risk of cardiovascular events and all-cause mortality: A meta-analysis of prospective cohort studies. Journal of the American Heart Association. 6(5): e005505. https://doi.org/10.1161/JAHA.117.005505.
Quirk, J. E. and Sinning, W. E. 1982. Anaerobic and aerobic responses of males and females to rope skipping. Medicine & Science in Sports & Exercise. 14(1): 26-29.
Riley, R. D., Ensor, J., Snell, K. I. E., Harrell Jr, F. E., Martin, G. P., Reitsma, J. B., Moons, K. G. M., Collins, G., and van Smeden, M. 2020. Calculating the sample size required for developing a clinical prediction model. British Medical Journal. 368: m441. https://doi.org/10.1136/bmj.m441.
Ross, R., Blair, S. N., Arena, R., Church, T. S., Després, J. P., Franklin, B. A., Haskell, W. L., Kaminsky, L. A., Levine, B. D., Lavie, C. ., et al. 2016. Importance of assessing cardiorespiratory fitness in clinical practice: A case for fitness as a clinical vital sign: A scientific statement from the American Heart Association. Circulation. 134(24): e653-e699. https://doi.org/10.1161/ CIR.0000000000000461.
Siahkouhian, M. 2009. Impact of height on the prediction of maximum oxygen consumption in active young men. Journal of Applied Sciences 9:2340-2343. https://doi.org/10.3923/jas.2009.2340.2343.
Takken, T., Mylius, C. F., Paap, D., Broeders, W., Hulzebos, H. J., Van Brussel, M., and Bongers, B. C. 2019. Reference values for cardiopulmonary exercise testing in healthy subjects—an updated systematic review. Expert Review of Cardiovascular Therapy. 17: 413-426. https://doi.org/10.1080/14779072.2019.1627874.
Town, G. F., Sol, N., and Sinning, W. E. 1980. The effect of rope skipping rate on energy expenditure of males and females. Medicine & Science in Sports & Exercise. 12(4): 295-298.
van der Steeg, G.E. and Takken, T. 2021. Reference values for maximum oxygen uptake relative to body mass in Dutch/Flemish subjects aged 6–65 years: The lowlands fitness registry. European Journal of Applied Physiology. 121: 1189-1196. https://doi.org/10.1007/s00421-021-04596-6.
Warburton, D. E. R., Jamnik, V., Bredin, S. S. D., Shephard, R. J., and Gledhill, N. 2018. The 2019 physical activity readiness questionnaire for everyone (PAR-Q+) and electronic physical activity readiness medical examination (ePARmed-X+): 2019 PAR-Q+. Health & Fitness Journal of Canada. 11(4): 80-83. https://doi.org/10.14288/hfjc.v11i4.270.
Wasserman, K., Hansen, J. E., Sue, D. Y., Stringer, W., and Whipp, B. J. 2005. Principles of exercise testing and interpretation. Lippincott Williams & Wilkins, Philadelphia.
Wilke, J. and Mohr, L. 2020. Chronic effects of high-intensity functional training on motor function: A systematic review with multilevel meta-analysis. Scientific Reports. 10: 21680. https://doi.org/10.1038/s41598-020-78615-5.
OPEN access freely available online
Natural and Life Sciences Communications
Chiang Mai University, Thailand. https://cmuj.cmu.ac.th
Chadaporn Khamjing1, Aujima Ngukhiew2, Abdulchukkri Kasemsah2, Supatcha Konghakote2, Pongson Yaicharoen3, and Sainatee Pratanaphon2,*
1 Sports Science Program, Chiang Mai University, Chiang Mai 50200, Thailand.
2 Department of Physical Therapy, Faculty of Associated Medical Sciences, Chiang Mai University, Chiang Mai 50200, Thailand.
3 Department of Physiology, Faculty of Medicine, Chiang Mai University, Chiang Mai 50200, Thailand.
Corresponding author: Sainatee Pratanaphon, E-mail: sainatee.pra@cmu.ac.th
Total Article Views
Editor: Waraporn Booncheng,
Chiang Mai University, Thailand
Article history:
Received: August 27, 2024;
Revised: December 8, 2024;
Accepted: December 11, 2024;
Online First: December 24, 2024