 ISSN: 2822-0838 Online
ISSN: 2822-0838 Online

Skeletal Growth Status Agreement in a Group of Thai Children and Adolescents: A Comparative Analysis of Fishman's Skeletal Maturation and Baccetti's Cervical Vertebral Maturation Indices
Witsarut Upalananda* , Aree Kanjanaprapas, and Udom ThongudompornPublished Date : March 12, 2024
DOI : https://doi.org/10.12982/NLSC.2024.025
Journal Issues : Number 2, April-June 2024
Abstract This study aimed to determine the agreement of skeletal maturation (SM) assessed by hand-wrist radiographs and cervical vertebral maturation (CVM) assessed by lateral cephalometric radiographs. It also explored the feasibility of using CVM as an alternative to hand-wrist radiographs among Thai children and adolescents. The samples comprised 95 males and 67 females from Thailand, aged 7–17 years. A total of 162 hand-wrist radiographs and lateral cephalometric radiographs were included. Two experienced oral radiologists independently assessed SM (using Fishman’s method) and CVM (using Baccetti’s method); a third referee observer resolved any discrepancies. The correlation and agreement between the methods were evaluated. The results found a substantial agreement (weighted kappa = 0.594) between SM and CVM. The interobserver discrepancy in categorizing SM stages was mostly found at stage 5, while the most common discrepancy for CVM was at stage 6. A significant positive correlation (Spearman’s correlation coefficient = 0.677, P < 0.001) indicated a moderate to strong association between SM and CVM. The substantial agreement and moderate to strong correlation between CVM and SM highlighted the feasibility of using CVM to assess skeletal growth. However, to ensure reliability, it was necessary to precisely evaluate the appearance of the capping of the epiphyseal plate for SM and the distinction between a rectangular and square cervical spine shape at C3 and C4 for CVM differentiation.
Keywords: Cervical spine, Hand, Radiographic evaluation, Orthodontics
Citation: Upalananda,W., Kanjanaprapas, A., and Thongudomporn, U. 2024. Skeletal growth status agreement in a group of Thai children and adolescents: A comparative analysis of Fishman's skeletal maturation and Baccetti's cervical vertebral maturation indices. Natural and Life Sciences Communications. 23(2): e2024025.
INTRODUCTION
Orthodontists assess the skeletal growth of adolescent patients to diagnose and plan treatments, especially during pubertal growth spurts. Chronological age cannot effectively indicate skeletal growth because of discrepancies in skeletal maturation (SM) between patients of the same age (Alkhal et al., 2008). Hand-wrist radiographs are highly effective at assessing SM and are commonly used to evaluate skeletal growth (Flores-Mir et al., 2004); however, this technique requires a dose of radiation.
Orthodontic patients receive routine lateral cephalometric radiographs as the standard imaging used in their treatment. These radiographs evaluate skeletal size, shape, and position, assess unerupted or ectopic teeth, and measure growth (Dreyer, 2008; Devereux et al., 2011). Several methods have been established to evaluate skeletal growth from lateral cephalometric radiographs that indicate cervical vertebral maturation (CVM); these are commonly used to assess jaw discrepancies (Hassel and Farman, 1995; Baccetti et al., 2002; 2005; Román et al., 2002) .Furthermore, orthodontic growth assessment methods often rely on references from previous investigations. Fishman’s study (Fishman, 1982) derived reference data from the Denver Child Research Council, collected between 1927 and 1967 (Maresh, 1970). Similarly, Baccetti’s study (Baccetti et al., 2005) used reference data from “An Atlas of Craniofacial Growth: Cephalometric Standards from The University School Growth Study, The University of Michigan” (Riolo et al., 1974). Consequently, evaluating growth status based on Fishman’s SM and Baccetti’s CVM indices implies that we determined growth status using references from these established baseline populations; however, previous evidence noted variations in skeletal growth among different ethnicities (Zhang et al., 2009; Cole et al., 2015; Schoenbuchner et al., 2017; Grgic et al., 2020).
Previous studies on the Thai population have explored the correlation between SM indices based on hand-wrist radiographs and dental calcification (Krailassiri et al., 2002), as well as the correlation between the CVM index based on lateral cephalometric radiographs and chronological age (Pisek et al., 2013). Yet, a comparative analysis of SM and CVM in a healthy Thai population remains absent. Therefore, this study aimed to determine the level of agreement between Fishman’s SM and Baccetti’s CVM indices in a group of Thai children and adolescents. Additionally, we assessed the feasibility of CVM as an alternative to hand-wrist radiographs for assessing skeletal growth, aiming to determine whether CVM is a viable alternative to SM for evaluating the growth status of Thai patients.
MATERIAL AND METHODS
Data collection
Ethical approval was obtained from The Human Research Ethics Committee, Faculty of Dentistry, Prince of Songkla University, Songkhla, Thailand (EC6504-023). The study was conducted in full compliance with the Declaration of Helsinki. The protocol was registered with the Thai Clinical Trial Registry (TCTR20230628005). The included samples were individuals of Thai nationality, aged 7–17, who had received hand-wrist radiographs and lateral cephalometric radiographs. The participants’ dates of birth and dates of radiography were recorded. The exclusion criteria were radiographs of poor image quality, radiographs that were not obtained on the same day, and patients who were diagnosed with conditions that could potentially impact their development. A total of 174 patients who received both lateral cephalometric radiographs and hand-wrist radiographs during the period spanning March 2018 to December 2021, were retrospectively selected and subsequently stored in digital format as JPEG files. Two imaging machines were used: a GXDP-700 (Gendex Dental Systems, Hatfield, Pennsylvania, USA) and an Orthopantomograph OP300 (Instrumentarium Dental, Charlotte, North Carolina, USA). After the exclusion criteria were applied, the final study sample was 162 participants. There were 95 male participants, with a mean age of 12.39 years and a standard deviation of 1.84 years. There were 67 female participants, with a mean age of 11.76 years and a standard deviation of 1.88 years. The distribution of the sample is given in Figure 1.
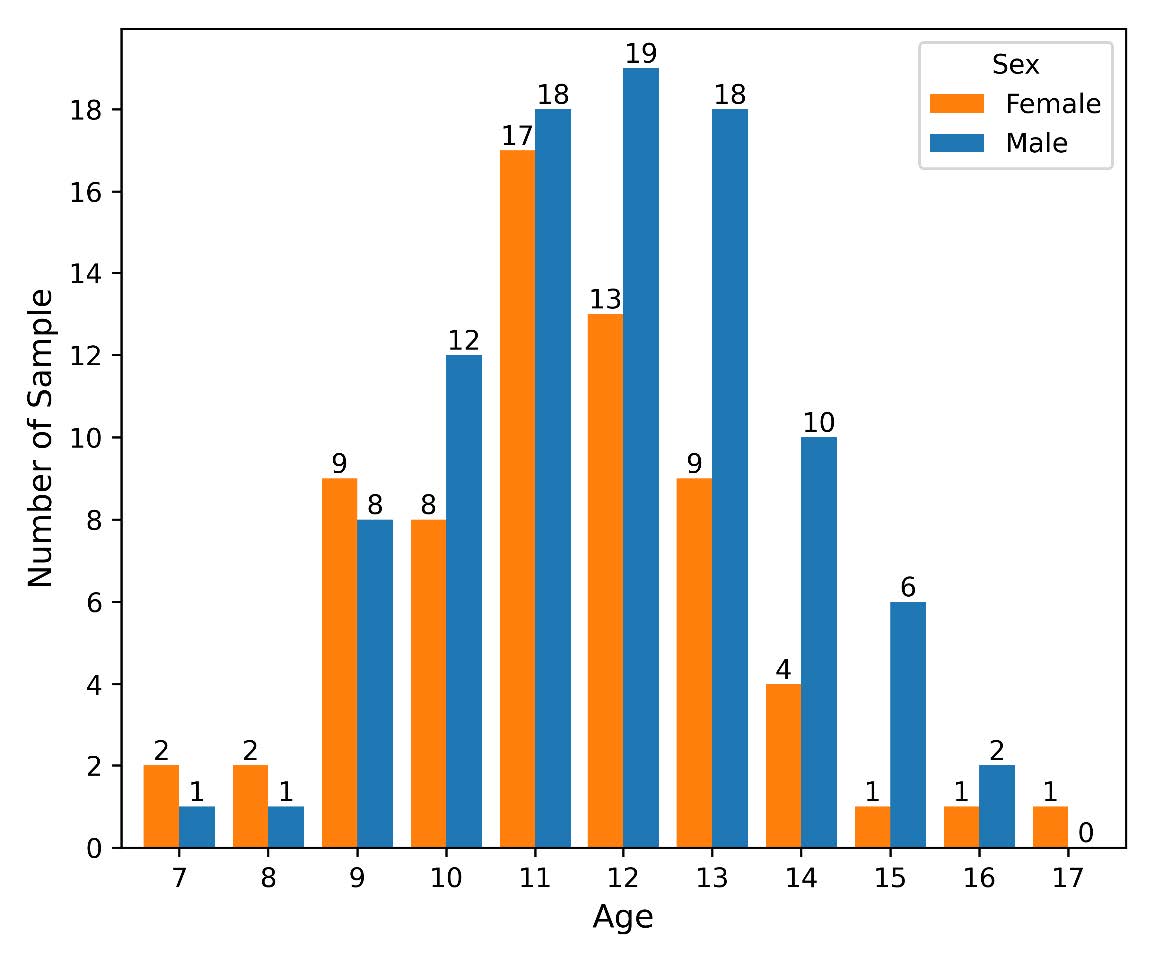
Figure 1. Distribution of age and sex of the samples.
Data preparation
The samples’ non-dominant hand-wrist radiographs and lateral cephalometric radiographs were extracted from the storage system. The observers were individually blinded to the images, which were annotated with identifying numbers. The demographic data of the patients were concealed. To mitigate bias in evaluating the lateral cephalometric radiographs, the images were cropped to only contain the region of the cervical vertebrae before assessment (Figure 2).

Figure 2. Examples of radiographic images. (a) Hand-wrist radiograph. (b) Cropped lateral cephalometric radiograph.
Radiographic assessment
The hand-wrist radiographs were used to assess the participants’ SM according to the 11 maturation stages of Fishman’s method (Table 1) (Fishman, 1982). The lateral cephalometric radiographs were used to assess CVM using Baccetti’s method, which defines cervical vertebra maturity in 6 stages (Table 2) (Baccetti et al., 2005).
Two oral radiologists (WU and AK) and one orthodontist (UT) conducted the assessment. Before the assessment, the three observers defined the SM and CVM assessment criteria to achieve mutual understanding. The two radiologists, who acted as the main observers, assessed the radiographs and assigned maturity stages separately; the results were then compared. The observers were given unlimited time to assess the radiographs; the SM and CVM assessment criteria were available during the assessment. Additionally, the observers were allowed to adjust the brightness and contrast of the radiographic images to allow clear evaluation. If the observers disagreed with their assessments, the third observer, certified by the Thai Board of Orthodontics and with over 25 years of experience in orthodontics, acted as a referee. The results from the main observers were used to evaluate the inter-observer reliability, while the results that had been reviewed by the referee were used for the analysis. Additionally, 30 samples were randomly selected to be re-evaluated a month after the first assessment by the main observers to determine the intra-observer reliability.
To evaluate the agreement between SM and CVM, Fishman’s SM stages were reclassified into three groups according to growth status: pre-peak (SM stages 1–4), peak (SM stages 5–7), and post-peak (SM stages 8–11) (Fishman, 1982). Baccetti’s CVM stages were also categorized as pre-peak (CVM stages 1–2), peak (CVM stages 3–4), and post-peak (CVM stages 5–6) (Baccetti et al., 2005).
Table 1. Fishman’s skeletal maturation stages (Fishman, 1982).
|
Stage |
Criteria |
|
1 |
“Width of epiphysis as wide as the diaphysis: Third finger – proximal phalanx” |
|
2 |
“Width of epiphysis as wide as the diaphysis: Third finger – middle phalanx” |
|
3 |
“Width of epiphysis as wide as the diaphysis: Fifth finger – middle phalanx” |
|
4 |
“Ossification: Adductor sesamoid of thumb” |
|
5 |
“Capping of epiphysis: Third finger – distal phalanx” |
|
6 |
“Capping of epiphysis: Third finger – middle phalanx” |
|
7 |
“Capping of epiphysis: Fifth finger – middle phalanx” |
|
8 |
“Fusion of epiphysis and diaphysis: Third finger – distal phalanx” |
|
9 |
“Fusion of epiphysis and diaphysis: Third finger – proximal phalanx” |
|
10 |
“Fusion of epiphysis and diaphysis: Third finger – middle phalanx” |
|
11 |
“Fusion of epiphysis and diaphysis: Radius” |
Table 2. Baccetti’s cervical vertebral maturation stages (Baccetti et al., 2005).
|
Stages |
Criteria |
|
1 |
“The lower borders of all the three vertebrae (C2–C4) are flat. The bodies of both C3 and C4 are trapezoid in shape (the superior border of the vertebral body is tapered from posterior to anterior).” |
|
2 |
“A concavity is present at the lower border of C2 (in four of five cases, with the remaining subjects still showing a cervical stage 1). The bodies of both C3 and C4 are still trapezoid in shape.” |
|
3 |
“Concavities at the lower borders of both C2 and C3 are present. The bodies of C3 and C4 may be either trapezoid or rectangular horizontal in shape.” |
|
4 |
“Concavities at the lower borders of C2, C3, and C4 now are present. The bodies of both C3 and C4 are rectangular horizontal in shape.” |
|
5 |
“The concavities at the lower borders of C2, C3, and C4 still are present. At least one of the bodies of C3 and C4 is squared in shape. If not square, the body of the other cervical vertebra still is rectangular horizontal.” |
|
6 |
“The concavities at the lower borders of C2, C3, and C4 still are evident. At least one of the bodies of C3 and C4 is rectangular vertical in shape. If not rectangular vertical, the body of the other cervical vertebra is squared.” |
Statistical analysis
The samples’ sex and chronological age distributions were ascertained with descriptive statistics. The intra- and inter-observer reliabilities were determined using Cohen’s weighted kappa coefficient (κ). A weighted κ measured the agreement between the groups of growth statuses according to SM and CVM stages. The magnitude of agreement according to κ was interpreted as either poor (< 0.00), slight (0.00–0.20), fair (0.21–0.40), moderate (0.41–0.60), substantial (0.61–0.80), or almost perfect (0.81–1.00) (Landis and Koch, 1977). The correlation between SM and CVM assessments was analyzed using Spearman’s rank correlation (α = 0.05). All statistical analyses were performed using Python version 3.10.9 in Jupyter Notebook. The NumPy, Pandas, SciPy, Sci-Kit Learn, and Matplotlib libraries were used for data analysis and visualization.
RESULTS
Observer reliability
The intra-observer reliabilities of Fishman’s method for observers WU and AK were in almost perfect agreement (κ = 0.99 and 0.98, respectively). The observers’ assessments of Baccetti’s method were also in almost perfect agreement at different time points (κ = 0.95 for WU and 0.99 for AK). Additionally, the inter-observer reliabilities of Fishman’s method and Baccetti’s method were in almost perfect agreement (κ = 0.98 and 0.96, respectively).
The term ‘discrepancy’ refers to differences in the two observers’ categorizations of maturation stages when assessing the same images. The distributions of SM and CVM stages, along with their corresponding assessment discrepancies, are provided in Tables 3 and 4, respectively. Among the 162 SM evaluations, 32 instances of discrepancies were identified. The highest discrepancy rate was found in SM stage 5 (60.00%), whereas there were no discrepancies in the assessments of SM stages 8 and 9. Moreover, 29 discrepancies had a one-stage difference, while two instances had a two-stage difference (in SM stages 1 and 6); one instance had a three-stage difference (in SM stage 10). There were 14 discrepancies out of 162 CVM assessments. CVM Stage 6 had the highest discrepancy rate of 33.33%. In contrast, CVM stage 3 assessments revealed no discrepancies. Additionally, the largest discrepancy observed in these cases was a two-stage difference (two occurrences in CVM stages 1 and 2), while the other 12 discrepancies were only a one-stage difference.
Table 3. Skeletal maturation assessment: distribution of total assessments and discrepancies for each stage.
|
SM stage |
Total assessment |
Discrepancy |
Discrepancy rate (%) |
|
1 |
19 |
4 |
21.05 |
|
2 |
12 |
3 |
25.00 |
|
3 |
20 |
7 |
35.00 |
|
4 |
7 |
1 |
14.29 |
|
5 |
5 |
3 |
60.00 |
|
6 |
24 |
7 |
29.17 |
|
7 |
37 |
2 |
5.41 |
|
8 |
11 |
0 |
0.00 |
|
9 |
2 |
0 |
0.00 |
|
10 |
21 |
4 |
19.05 |
|
11 |
4 |
1 |
25.00 |
|
Total |
162 |
32 |
19.75 |
Table 4. Cervical vertebral maturation assessment: distribution of total assessments and discrepancies for each stage.
|
CVM stage |
Total assessment |
Discrepancy |
Discrepancy rate (%) |
|
1 |
7 |
1 |
14.29 |
|
2 |
31 |
4 |
12.90 |
|
3 |
23 |
0 |
0.00 |
|
4 |
51 |
3 |
5.88 |
|
5 |
41 |
3 |
7.32 |
|
6 |
9 |
3 |
33.33 |
|
Total |
162 |
14 |
8.64 |
Correlation and agreement between SM and CVM
The findings of the study indicated a statistically significant and positive association between Fishman’s SM and Baccetti’s CVM. The correlation coefficient between the variables was 0.677 (P < 0.001), suggesting a significant, moderately strong, and positive relationship. Additionally, stratification by sex demonstrated that both the male and female subgroups exhibited notable positive associations, with correlation coefficients of 0.652 (P < 0.001) and 0.724 (P < 0.001), respectively.
The agreement between SM and CVM is given in Table 5. The weighted kappa value of the groups of growth status, categorized as pre-peak, peak, and post-peak, according to SM and CVM stages was 0.594, indicating moderate agreement. The sex-specific agreements were 0.571 and 0.614 for males and females, respectively.
Table 5. Cross-tabulation of skeletal and cervical vertebral maturation by sex.
|
Sex |
Skeletal maturation |
Cervical vertebral maturation |
Total |
||
|
Pre-peak (Baccetti’s Stage 1–2) |
Peak (Baccetti’s Stage 3–4) |
Post-peak (Baccetti’s Stage 5–6) |
|||
|
Male |
Pre-peak |
18 |
20 |
2 |
40 |
|
Peak (Fishman’s Stage 5–7) |
3 |
25 |
10 |
38 |
|
|
Post-peak (Fishman’s Stage 8–11) |
0 |
4 |
13 |
17 |
|
|
Total |
21 |
49 |
25 |
95 |
|
|
Female |
Pre-peak |
11 |
6 |
1 |
18 |
|
Peak (Fishman’s Stage 5–7) |
5 |
15 |
8 |
28 |
|
|
Post-peak (Fishman’s Stage 8–11) |
1 |
4 |
16 |
21 |
|
|
Total |
17 |
25 |
25 |
67 |
|
DISCUSSION
Numerous studies have investigated growth assessment indices in Thai populations. Krailassiri et al. (2002) found significant relationships between dental calcification stages and SM, with a Spearman’s rank correlation coefficient of 0.31–0.69. Pisek et al. (2013) reported a high correlation between CVM and chronological age, with a Spearman’s rank correlation coefficient of 0.77. Additionally, Theerasopon et al. (2022) observed that dental age closely approximated chronological age within a year for both sexes. This study investigated methods of assessing SM in healthy Thai adolescents. A substantial level of agreement was found between Fishman’s SM and Baccetti’s CVM assessment methods. Previous studies on the agreement between SM and CVM in different populations reported various levels of agreement; substantial to almost perfect agreements were observed in studies of Italian populations (Gandini et al., 2006; Pasciuti et al., 2013) and Indian populations (Chalasani et al., 2013; Prasad et al., 2013; Pichai et al., 2014). These findings are consistent with this study, which demonstrated a substantial level of agreement. However, a study of an Iranian population revealed only a fair agreement between SM and CVM (Hoseini et al., 2016), which emphasizes the variability in agreement levels across diverse populations.
A previous study revealed a κ = 0.80 agreement between SM and CVM methods in Thai cleft patients – a higher agreement than this study that was still categorized as substantial (Manosudprasit et al., 2013). This difference might be caused by different growth rates in the healthy population and cleft patients (Ravi and Ravikala, 2013; Batwa et al., 2018). The CVM assessment methods were also different; previous studies used Hassel and Farman’s method to determine CVM (Hassel and Farman, 1995), while this study employed Baccetti’s method.
Determining skeletal growth is crucial for orthodontists to identify the optimal timing of treatment, particularly for the efficient correction of occlusal anomalies associated with growth (Fleming, 2017). The assessment of growth stages conventionally involves categorizing the patient’s skeletal growth into pre-peak, peak, and post-peak phases. This study evaluated skeletal growth with two distinct methods: Fishman’s and Baccetti’s. Fishman’s method assessed SM with hand-wrist radiographs, considering statural height, maxillary growth, and mandibular growth (Fishman, 1982). Conversely, Baccetti’s method evaluated CVM from lateral cephalometric radiographs, focusing on determining mandibular growth based on total mandibular length (Baccetti et al., 2005). The distinct skeletal indices used in the assessments may have contributed to variations in the level of agreement between the two methods. Therefore, this study investigated the growth assessment consistency of the two methods, ensuring accurate interpretation of growth assessment and enhancing confidence in determining the optimal duration of orthodontic treatments.
This study reported differences in the degree of SM and CVM agreement between males and females, with females having a higher agreement than males. A higher agreement in females was also reported in previous studies (San Román et al., 2002; Manosudprasit et al., 2013; Prasad et al., 2013; Danaei et al., 2014). These findings correspond to earlier studies, which revealed sex differences in the timing of early CVM stages (Montasser et al., 2017). Therefore, using CVM to assess SM may be more reliable in females than in males. Furthermore, the results revealed a tendency for a more advanced CVM growth status in males compared to the growth status of SM. This suggested a potential trend of overestimating growth assessment using CVM in the male population.
Hand-wrist radiographs are primarily used to predict growth, which is important for planning orthodontic treatments (Verma et al., 2009). The limitation of this method is that it requires additional exposure to ionizing radiation. It would, therefore, be beneficial to use lateral cephalometric radiographs, which are routinely prescribed for orthodontic treatment, to predict growth based on CVM (Lucchese et al., 2022). This study reported high intra- and inter-observer reliability in both methods, which indicates their applicability in clinical practice.
The findings have significant clinical implications for radiographic evaluation of SM and CVM in orthodontics. The highest discrepancy rate was observed in assessing SM using Fishman’s method (Fishman, 1982), at SM stage 5. This highlights the challenges associated with assessing whether the epiphyseal plate is capping. Additionally, the discrepancy rate in assessing CVM with Baccetti’s method (Baccetti et al., 2005) was the highest at CVM stage 6. This discrepancy was related to the evaluation of the shape of the cervical spine at C3 and C4, specifically regarding whether it was rectangular vertical, or square. Orthodontic practitioners should be mindful of these criteria to ensure that assessments in clinical practice are accurate.
Despite its valuable findings, this study had certain limitations. Although the cross-sectional study analyzed the agreement between SM and CVM assessments in Thai children and adolescents, it did not directly investigate the relationship between CVM and jawbone development. Even though SM, based on hand-wrist radiograph analysis, was the best indicator for the peak growth velocity evaluation, some errors were still present in the method (Mellion et al., 2013). Furthermore, the lack of longitudinal reference data specific to the growth patterns of the jawbone of the Thai population limits the authentic appraisal of the growth status of Thais. Future longitudinal studies should aim to explore SM, CVM, and jawbone development of the Thai population simultaneously.
Additionally, the dataset primarily included samples who were candidates for growth modification treatment. Ethical considerations prevented the inclusion of patients who were either too young or too old, as they were not prescribed hand-wrist radiographs for unnecessary growth assessment. This ethical issue resulted in an uneven dataset distribution, prompting considerations for potential research limitations. It is also essential to acknowledge that the samples were collected from a single location. To enhance the generalizability of the results to the broader Thai population, a multicenter analysis should be undertaken. Additionally, investigating any direct connection between CVM and jawbone development in future research would provide further insights into the orthodontic implications of these assessments.
CONCLUSION
In conclusion, this study revealed a substantial agreement between SM and CVM assessment methods in a group of Thai children and adolescents. The results highlighted the need to consider the degree of inconsistency between these methods in clinical applications. While both Fishman’s and Baccetti’s methods were highly reliable, a notable number of interobserver discrepancies were observed at specific stages. These challenges were most evident in evaluating the capping of the epiphyseal plate and the shape of the cervical spine at C3 and C4; therefore, caution should be exercised when using either method to assess these stages.
ACKNOWLEDGEMENTS
The authors are grateful to the staff of the Radiology Clinic, Faculty of Dentistry, Prince of Songkla University for assisting in data collection.
AUTHOR CONTRIBUTIONS
Witsarut Upalananda performed the conceptualization, project administration, methodology, data collection, validation, investigation, formal analysis, visualization, and writing. Aree Kanjanaprapas participated in the methodology, investigation, and writing. Udom Thongudomporn took part in the methodology, investigation, formal analysis, supervision, and writing. All authors have read and approved the final manuscript.
CONFLICTS OF INTEREST
The authors declare that they hold no competing interests.
REFERENCES
Alkhal, H.A., Wong, R.W., and Rabie, A.B.M. 2008. Correlation between chronological age, cervical vertebral maturation and fishman's skeletal maturity indicators in southern Chinese. The Angle Orthodontist. 78(4): 591-596.
Baccetti, T., Franchi, L., and McNamara, Jr J.A. 2002. An improved version of the cervical vertebral maturation (CVM) method for the assessment of mandibular growth. The Angle Orthodontist. 72(4): 316-323.
Baccetti, T., Franchi, L., and McNamara, Jr J.A. 2005. The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Seminars in Orthodontics. 11(3): 119-129.
Batwa, W., Almoammar, K., Aljohar, A., Alhussein, A., Almujel S., and Zawawi, K.H. 2018. The difference in cervical vertebral skeletal maturation between cleft lip/palate and non-cleft lip/palate orthodontic patients. Biomed Research International. 2018: 5405376.
Chalasani, S., Kumar, J., Prasad, M., Shetty, B.S.K., and Kumar, T.A. 2013. An evaluation of skeletal maturation by hand-wrist bone analysis and cervical vertebral analysis: A comparitive study. Journal of Indian Orthodontic Society. 47(4_suppl4): 433-437.
Cole, T.J., Rousham, E.K., Hawley, N.L., Cameron, N., Norris, S.A., and Pettifor, J.M. 2015. Ethnic and sex differences in skeletal maturation among the birth to twenty cohort in south Africa. Archives of Disease in Childhood. 100(2): 138-143.
Danaei, S.M., Karamifar, A., Sardarian, A., Shahidi, S., Karamifar, H., Alipour, A., and Ghodsi Boushehri, S. 2014. Measuring agreement between cervical vertebrae and hand-wrist maturation in determining skeletal age: Reassessing the theory in patients with short stature. American Journal of Orthodontics and Dentofacial Orthopedics. 146(3): 294-298.
Devereux, L., Moles, D., Cunningham, S.J., and McKnight, M. 2011. How important are lateral cephalometric radiographs in orthodontic treatment planning? American Journal of Orthodontics and Dentofacial Orthopedics. 139(2): e175-e181.
Dreyer, C. 2008. Orthodontic radiographs. Guidelines, 3rd ed. (2008). European Journal of Orthodontics. 30(6): 669-670.
Fishman, L.S. 1982. Radiographic evaluation of skeletal maturation. A clinically oriented method based on hand-wrist films. The Angle Orthodontist. 52(2): 88-112.
Fleming, P. 2017. Timing orthodontic treatment: Early or late? Australian Dental Journal. 62(S1): 11-19.
Flores-Mir, C., Nebbe, B., and Major, P.W. 2004. Use of skeletal maturation based on hand-wrist radiographic analysis as a predictor of facial growth: A systematic review. The Angle Orthodontist. 74(1): 118-124.
Gandini, P., Mancini, M., and Andreani, F. 2006. A comparison of hand-wrist bone and cervical vertebral analyses in measuring skeletal maturation. The Angle Orthodontist. 76(6): 984-989.
Grgic, O., Shevroja, E., Dhamo, B., Uitterlinden, A.G., Wolvius, E.B., Rivadeneira, F., and Medina-Gomez, C. 2020. Skeletal maturation in relation to ethnic background in children of school age: The generation R study. Bone. 132: 115180.
Hassel, B. and Farman, A.G. 1995. Skeletal maturation evaluation using cervical vertebrae. American Journal of Orthodontics and Dentofacial Orthopedics. 107(1): 58-66.
Hoseini, M., Zamaheni, S., Fakhar, H.B., Akbari, F., Chalipa, J., and Rahmati, A. 2016. Comparative evaluation of the efficacy of hand-wrist and cervical vertebrae radiography for the determination of skeletal age. Iranian Journal of Radiology. 13(3): e21695.
Krailassiri, S., Anuwongnukroh, N., and Dechkunakorn, S. 2002. Relationships between dental calcification stages and skeletal maturity indicators in Thai individuals. The Angle Orthodontist. 72(2): 155-166.
Landis, J.R. and Koch, G.G. 1977. The measurement of observer agreement for categorical data. Biometrics. 159-174.
Lucchese, A., Bondemark, L., Farronato, M., Rubini, G., Gherlone, E.F., Lo Giudice, A., and Manuelli, M. 2022. Efficacy of the cervical vertebral maturation method: A systematic review. Turkish Journal of Orthodontics. 35(1): 55-66.
Manosudprasit, M., Wangsrimongkol, T., Pisek, P., and Chantaramungkorn, M. 2013. Comparative study between the hand-wrist method and cervical vertebral maturation method for evaluation skeletal maturity in cleft patients. Journal of the Medical Association of Thailand. 96 Suppl 4: S19-24.
Maresh, M.M. 1970. Measurements from roentgenograms, heart size, long bone lengths, bone, muscles and fat widths, skeletal maturation. p 155–200. In McCammon, R.W., (ed) Human growth and development. Charles C. Thomas, Springfield, Illinois.
Mellion, Z.J., Behrents, R.G., and Johnston, L.E. 2013. The pattern of facial skeletal growth and its relationship to various common indexes of maturation. American Journal of Orthodontics and Dentofacial Orthopedics. 143(6): 845-854.
Montasser, M.A., Viana, G., and Evans, C.A. 2017. Racial and sex differences in timing of the cervical vertebrae maturation stages. American Journal of Orthodontics and Dentofacial Orthopedics. 151(4): 744-749.
Pasciuti, E., Franchi, L., Baccetti, T., Milani, S., and Farronato, G. 2013. Comparison of three methods to assess individual skeletal maturity. Journal of Orofacial Orthopedics. 5: 397-408.
Pichai, S., Rajesh, M., Reddy, N., Adusumilli, G., Reddy, J., and Joshi, B. 2014. A comparison of hand wrist bone analysis with two different cervical vertebral analysis in measuring skeletal maturation. Journal of International Oral Health. 6(5): 36-41.
Pisek, P., Godfrey, K., Manosudprasit, M., Wangsrimongkol, T., and Leelasinjaroen, P. 2013. A comparison of cervical vertebral maturation assessment of skeletal growth stages with chronological age in Thai between cleft lip and palate and non-cleft patients. Journal of the Medical Association of Thailand. 96 Suppl 4: S9-18.
Prasad, M., Ganji, V.S.K., George, S.A., Talapaneni, A.K., and Shetty, S.K. 2013. A comparison between cervical vertebrae and modified mp3 stages for the assessment of skeletal maturity. Journal of Natural Science, Biology and Medicine. 4(1): 74-80.
Ravi, M. and Ravikala, S. 2013. Assessment of skeletal age in children with unilateral cleft lip and palate. International Journal of Clinical Pediatric Dentistry. 6(3): 151-155.
Riolo, M.L., Moyers, R.E., McNamara, J.A., and Hunter, W.S. 1974. An atlas of craniofacial growth: Cephalometric standards from the university school growth study, the university of Michigan. Center for Human Growth and Development, the University of Michiagan, Ann Abor, Michigan.
Román, P.S., Palma, J.C., Oteo, M.D., and Nevado, E. 2002. Skeletal maturation determined by cervical vertebrae development. European Journal of Orthodontics. 24(3): 303-311.
Schoenbuchner, S.M., Pettifor, J.M., Norris, S.A., Micklesfield, L.K., Prentice, A., and Ward, K.A. 2017. Ethnic differences in peripheral skeletal development among urban south African adolescents: A ten‐year longitudinal PQCT study. Journal of Bone and Mineral Research. 32(12): 2355-2366.
Theerasopon, P., Tiansuwan, K., Srichaitan, N., Norkaew, S., Charoemratrote, C., Srimaneekarn, N., and Duangto, P. 2022. Testing the accuracy of an age estimation method using radiographs of permanent mandibular third molar teeth in a Thai population. Chiang Mai University Journal of Natural Sciences. 21(3): e2022045.
Verma, D., Peltomäki, T., and Jäger, A. 2009. Reliability of growth prediction with hand–wrist radiographs. European Journal of Orthodontics. 31(4): 438-442.
Zhang, A., Sayre, J.W., Vachon, L., Liu, B.J., and Huang, H. 2009. Racial differences in growth patterns of children assessed on the basis of bone age. Radiology. 250(1): 228-235.
OPEN access freely available online
Natural and Life Sciences Communications
Chiang Mai University, Thailand. https://cmuj.cmu.ac.th
Witsarut Upalananda1,*, Aree Kanjanaprapas1, and Udom Thongudomporn2
1 Section of Oral and Maxillofacial Radiology, Department of Oral Diagnostic Sciences, Faculty of Dentistry, Prince of Songkla University, Songkhla 90110, Thailand.
2 Orthodontic Section, Department of Preventive Dentistry, Faculty of Dentistry, Prince of Songkla University, Songkhla 90110, Thailand.
Corresponding author: Witsarut Upalananda, E-mail: witsarut.u@psu.ac.th
Total Article Views
Editor: Anak Iamaroon,
Chiang Mai University, Thailand
Article history:
Received: October 3, 2023;
Revised: January 16, 2024;
Accepted: March 6, 2024;
Online First: March 12, 2024