 ISSN: 2822-0838 Online
ISSN: 2822-0838 Online

Efficacy of Knee Acupuncture added Sanyinjiao Point for Patients with Knee Osteoarthritis Through Attenuated Systemic Inflammations
Warangkhana Klajing, Natticha Sumneang, Yin Shen Tan, Pongnared Jaengpromma, and Anongporn Kobroob*Published Date : July 10, 2023
DOI : https://doi.org/10.12982/NLSC.2023.051
Journal Issues : Number 3, July-September 2023
Abstract Osteoarthritis (OA) is a progressive degradation of the cartilage that is strongly linked to the inflammation, and resulting in pain, stiffness, and loss of mobility. Currently, interventions aimed at reducing inflammation, alleviating pain, and enhancing joint mobility are recommend in patients with OA. Although intervention with traditional acupuncture has been shown to reduce pain, inflammation, and improve knee motion, the effects of acupuncture added Sanyinjiao (SP6) point on pain, inflammation and knee motion have never been investigated in patients with knee OA. Twenty-three patients with knee OA were subjected to receive acupuncture added SP6 twice a week for five weeks (totaling ten sessions). Patients were assessed at baseline and after ten sessions of acupuncture added SP6 using knee range of motion measurement, modified Western Ontario and McMaster Universities OA Index, numerical rating scale, and systemic inflammation levels. After the end of treatment, the knee pain was significantly reduced in patients when compared to baseline (P < 0.001). Addition to improvement in knee pain, knee flexion and extension also showed significant improved compared to baseline (P < 0.001). Furthermore, the low-grade systemic inflammation levels were decreased in patients when compared to baseline (P < 0.001). Therefore, this is the first study to show that acupuncture added SP6 point provides the beneficial effects on pain and inflammation, improving knee motion in patients with knee OA.
Keywords: Acupuncture, Inflammation, Knee motion, Knee osteoarthritis, Pain, Chinese medicine
Funding: This work was supported by the Thailand science research and innovation fund and the University of Phayao [grant number FF64-RIM035 (AK)]; the School of Medical Science, University of Phayao, Phayao, Thailand [grant number MS221003 (AK)]; and the Unit of Excellent of Public Health [grant number PHUPUoE 02/2565 (WK)].
Citation: Klajing, W., Sumneang, N., Tan, Y.S., Jaengpromma, P., and Kobroob, A. 2023. Efficacy of knee acupuncture added sanyinjiao point for patients with knee osteoarthritis through attenuated systemic inflammations. Natural and Life Sciences Communications. 22(3): e2023051.
INTRODUCTION
The number of elderly people is gradually increasing worldwide. According to a report from the World Health Organization, this number will increase by 1.4 to 2.1 billion people between 2030 and 2050 (Rudnicka et al., 2020). Osteoarthritis (OA), a degenerative joint disease that belongs to the musculoskeletal disorders, is among the top ten causes of disability worldwide and also correlates positively with elderly (Gupta et al., 2005; Li and Chen, 2019; Minetto et al., 2020). OA occurs in several joints (e.g., knee, hip, and hand); however, it is most common in the knee, followed by the hand and the hip (Leifer et al., 2022). Knee OA is a joint disease of the knee due to wear and progressive loss of articular cartilage (Hsu and Siwiec, 2023). Its symptoms include knee pain, tenderness, decreased range of motion (ROM), crepitus, an occasional effusion, and often inflammation of varying degrees (Wilkins and Phillips, 2008). Since knee OA has been known to cause functional limitations, it is considered a significant contributor to the socioeconomic burden (Lee et al., 2021). Therefore, therapeutic strategies that alleviate the complications associated with knee OA could benefit not only the health, but also in socioeconomic status of the elderly.
Currently, there are optional treatments for knee OA, which include pharmacologic and surgical approaches (Wilkins and Phillips, 2008); however, the comprehensive therapeutic strategies remain limited due to their relatively high toxicity, cost, and possible complications (Karsdal et al., 2016). Previous evidence has been reported that treatment with non-steroid anti-inflammatory drugs can cause gastrointestinal side-effects (Karsdal et al., 2016; Schell et al., 2017); however, it is considered to be the most effective treatment for total knee replacement only in the end-stage of knee OA (Feng et al., 2018). Furthermore, knee replacement therapy can cause chronic pain and a limitation of mobility after surgery (Feng et al., 2018; Chew et al., 2019). Therefore, given the relatively low adverse effects and complications, alternative treatments that can relieve pain, improve ROM, and improve quality of life without suffering from knee osteoarthritis, are recommended by clinical guidelines as the first-line treatment for knee OA (Bennell et al., 2007).
Chronic low-grade inflammation is considered a major cause of progressive joint degeneration, including knee OA (Berenbaum, 2013). Therefore, therapeutic interventions which could decrease inflammation levels might relieve pain and result in an improvement of ROM in knee OA. There is growing evidence that Complementary and Alternative Medicine (CAM), which includes practices and herbal medicines, is gaining popularity and being used by people around the world for its positive effects such as anti-inflammation and pain relief (Rao et al., 1999; Brien et al., 2011; Wang, 2013; Seyed Hashemi et al., 2021; Phutrakool and Pongpirul, 2022). In addition, Acupuncture, an ancient practice of traditional Chinese medicine, one of the most widely accepted CAMs, has been reported to be able to relieve pain and improve knee motion in patients with knee OA (Tang et al., 2018; Teixeira et al., 2018; Korostyshevskiy, 2020). Previous studies have reported that traditional knee acupuncture could reduce pain and improve knee motion in patients with knee OA (Tang et al., 2018; Teixeira et al., 2018; Korostyshevskiy, 2020). Interestingly, Sanyinjiao (SP6) acupoint, a spot in the spleen channel, which functions as an important, general tonification point, was indicated in many disorders, including dysmenorrhea, allergies, immunological disease, and pain control (da Silva et al., 2011; Liu et al., 2013; Dincer and Oskay, 2021). Nonetheless, the efficacy of acupuncture added SP6 point on knee pain, knee motion, and inflammation levels in knee OA, has not been investigated. Thus, we investigated the effects of acupuncture added SP6 on knee pain, knee motion, and inflammation levels in elderly patients with knee OA. In this study, we hypothesized that acupuncture added SP6 point improves the motion of knee joint by alleviating knee pain and reducing inflammation in elderly patients with knee OA.
MATERIALS AND METHODS
Study design and ethical approval
This cross-sectional study was approved by the Ethics Committee at the University of Phayao, Thailand (certificate of approval, UP-HEC 1.3/037/64). It was carried out in accordance with the relevant rules and legislation. Medical records and the computerized hospital database of the Tambon Ban Thom Health Promoting Hospital were used to collect the data.
Identification of subjects
Inclusion criteria
All patients with knee OA attending the outpatient clinics of Tambon Ban Thom Health Promoting Hospital who met the following criteria were eligible for enrollment: (1) aged 60 years or over with a diagnosis of either one or both knee OA; and (2) clinical sign of knee OA using the American College of Rheumatology (ACR) criteria (Paul et al., 2023).
Participants with clinical knee OA were assessed using the ACR criteria. The decision tree format of the ACR classification criteria (Peat et al., 2006) for clinical knee osteoarthritis was used. The ACR clinical criteria for knee OA was fulfilled in the following circumstances:
crepitus + and morning stiffness >30 mins and bony enlargement +; or
crepitus + and morning stiffness ⩽30 mins; or
crepitus − and bony enlargement + (where + = present, − = absent).
Exclusion criteria
The exclusion criteria were as follows: (1) a history of knee arthroplasty; (2) a history of steroid or anti-inflammation agents within 6 months; (3) inability to move; and (4) poor communication or inability to communicate with questioners.
Knee acupuncture procedure
The acupuncture of the knee was standardized throughout this study by the physician acupuncturist, who had received training in the People's Republic of China. The acupoints used in this study were according to The Name and Location of Acupoints, issued in 2006 (GB/T 12346-2006) which as followed:1) Dubi (ST35) or Waixiyan located in a depression lateral to the patellar ligament; 2) Neixiyan (EX-LE5), located in the center of the depression of the patellar ligament opposite to ST35; 3) ST35, located in the center of the depression of the patellar ligament opposite to EX-LE5; 4) Heding (EX-LE2), located in the depression above the midpoint of the superior patellar border; 5) Yinlingquan (SP9), located in the depression between the lower border of the medial condyle of the tibia and the medial border of the tibia; 6) Yanglingquan (GB 34), located in the depression anterior and inferior to the head of the fibula, and 7) SP6, located medially four-finger wide above the ankle (Dincer & Oskay, 2021; Liu et al., 2013). Typically, SP6 is commonly used for both acupuncture and acupressure, and has been shown to offer relief from gynecologic disorders, including dysmenorrhea (Dincer & Oskay, 2021; Liu et al., 2013).
The disposable acupuncture needles (Φ0.25 × 40 mm; Suzhou Dongbang Acupuncture Inc., Suzhou, China, 215144) were inserted vertically to a depth of 1–2 mm after sterilization of the target acupoints. Then, the needles were manipulated using techniques, including lifting, thrusting, twisting, and rotating (Sangdee et al., 2002). Patients were treated twice a week (Tuesday and Friday) for 5 weeks, totaling ten sessions.
Study variables and measurement
Knee pain and function
Knee Pain and Function was assessed by the modified Thai version of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) (Goggins et al., 2005; Kuptniratsaikul & Rattanachaiyanont, 2007). The WOMAC is a self-reported protocol to assess pain, stiffness, and function of the lower extremity by specific 22 questions in a Thai version: 15 on physical function, 5 on pain, and 2 on stiffness. Each query has ten answer choices ranging from 0 (no, without difficulty, or no symptom) to 10 (unable to engage in activities or extreme symptoms). The WOMAC (Thai version) contains subtotal scores for pain ranging from 0 to 50, stiffness from 0 to 20, and function from 0 to 150. The total summation of WOMAC scores (Thai version) ranges from 0 to 220.
Numerical rating scale
Pain was assessed using a numerical rating scale (NRS). The NRS, a one-dimensional scale for rating pain intensity, ranges from 0 for “no pain” to 10 for “worst pain imaginable” (Jensen et al., 1986).
Range of knee motion
According to knee ROM, including knee flexion and extension, were measured using goniometer. The ROM was measured before and after each treatment session.
Plasma inflammatory marker
The plasma inflammatory markers, including the plasma Erythrocyte Sedimentation Rate (ESR) and high sensitivity C-Reactive Protein (hs-CRP) levels, were determined. Blood samples were collected prior to the treatment of the first session as baseline, and again after the tenth session of treatment. Plasma inflammatory markers were determined from all blood samples by ELISA.
Statistical analysis
Data were expressed as the mean ± standard deviation (S.D.). Data were analyzed using GraphPad Prism 9.3 software. Paired t-test was used to test the difference between before and after treatment. A P-value less than 0.05 was considered as a statistically significance.
RESULTS
Demographic data of all participants
A total of 23 patients with knee OA were enrolled and included in this study. Regarding 23 patients: 21.7% were male and the mean ± S.D. of age was 66.43 ± 5.62 years old. The mean ± S.D. of body weight and height were 58.95 ± 7.56 kilograms and 155.09 ± 8.40 centimeters, respectively (Table 1).
At baseline, the average of Modified Thai version WOMAC scores for physical function, pain, and stiffness were 94.22 ± 33.05, 29.39 ± 11.88, and 11.83 ± 5.74, respectively. The summation of WOMAC scores was 142.26 ± 34.24, indicating that all patients were limited in physical function, pain, and stiffness (Table 1).
Table 1. Demographic data of all participants.
|
Parameters |
N = 23 |
|
Clinical parameters |
|
|
Age (years) |
66.43 ± 5.62 |
|
Male, n (%) |
5 (21.7%) |
|
Weight (kg) |
58.95 ± 7.56 |
|
Hight (cm) |
155.09 ± 8.40 |
|
WOMAC Score |
|
|
Physical function index |
94.22 ± 33.05 |
|
Pain index |
29.39 ± 11.88 |
|
Stiffness index |
11.83 ± 5.74 |
|
Total score |
142.26 ± 34.24 |
Note: Data are presented as mean ± SD. WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index.
Effects of acupuncture on knee pain
According to pain intensity based on the NRS at baseline, the NRS ranged from 4 to 10, with an average of 7.67 ± 2.02. At the end of each treatment session, the pain reported by patient was decreased. Interestingly, the pain intensity was also gradually decreased when compared to their prior session (Figure 1A). In addition, at the end of the treatment, the pain was significantly decreased compared to pain at baseline (0.1 ± 0.4 vs. 7.67 ± 2.02, P < 0.001) (Figure 1B)
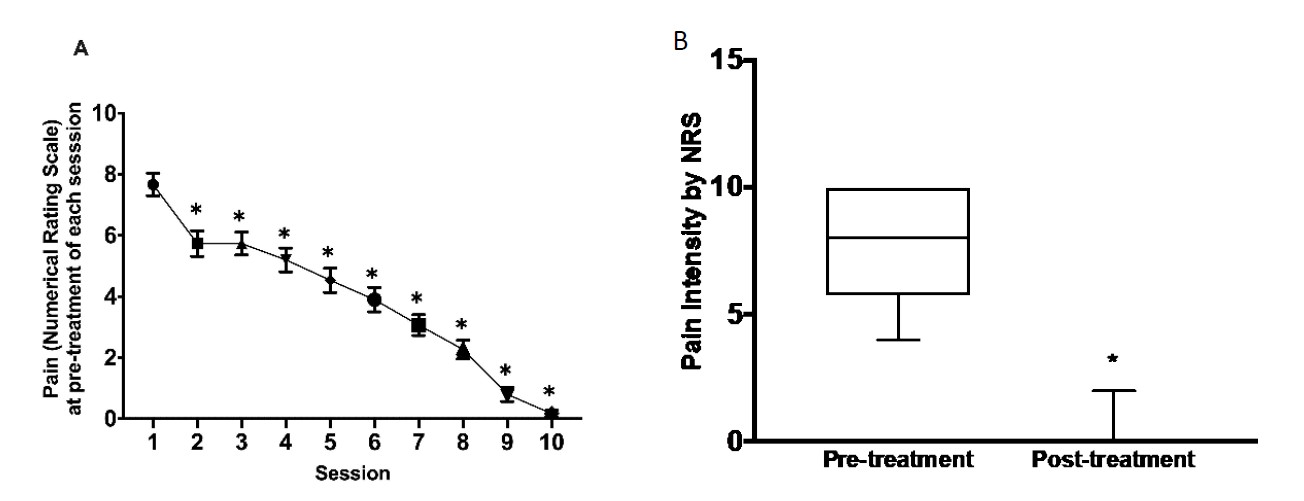
Figure 1. Effects of Acupuncture on knee pain using NRS. (A) overall pain intensity and (B) pain intensity. *P <0.05 vs. baseline. NRS: numerical rating scale.
Effects of acupuncture on knee motion
The knee flexion and extension were measured to determine the knee ROM. At the baseline level, the degree of knee flexion and extension were 103.4 ± 17.27 and -2.21 ± 1.47 degree, respectively. At the end of the treatment knee flexion was significantly increased when compared to baseline (131.4 ± 9.28 vs. 103.4 ± 17.27, P < 0.001). In addition, knee extension was also increased when compared to baseline (0.00 ± 0.37 vs. -2.21 ± 1.47, P < 0.001) as shown in Figure 2A and 2B.

Figure 2. Effects of Acupuncture on knee motion. (A) knee flexion, and (B) knee extension. *P <0.05 vs. baseline.
Effects of acupuncture on plasma inflammations
Plasma ESR and hs-CRP levels were determined at the baseline and at the end of treatment session. Treatment with acupuncture added SP6 point for ten sessions, plasma ESR and hs-CRP were significantly decreased when compared to their baseline levels (31.02 ± 28.13 vs. 100.00 and 34.98 ± 21.85, respectively, P < 0.001) as shown in Figure 3A and 3B

Figure 3. Effects of Acupuncture on inflammation. (A) plasma ESR level, and (B) Plasma hs-CRP level. *P <0.05 vs. baseline.
DISCUSSION
OA is reported to be a health and socioeconomic burden, and its incidence is increasing in many countries (Kiadaliri et al., 2017). Therefore, therapeutic strategies that alleviated the complications associated with knee OA could be beneficial to health and socioeconomic status. Since growing evidence reported that low-grade inflammation causing pain is strongly link to OA (Attur et al., 2015; Robinson et al., 2016), together with there is no disease-modifying treatment for knee OA, an alternative treatment by acupuncture is an option due to its ability to control pain and improve knee ROM (Tang et al., 2018; Teixeira et al., 2018; Korostyshevskiy, 2020). Interestingly, SP6 acupoint has been shown to be beneficial in various conditions, such as dysmenorrhea, immunological disease, and pain control (da Silva et al., 2011; Liu et al., 2013; Dincer and Oskay, 2021). However, the therapeutic efficacy of knee acupuncture added SP6 acupoint on pain and inflammations levels in elderly patients with knee OA are unknown. This study is the first investigated the effects of knee acupuncture added SP6 acupoint on knee pain, knee motion, and inflammation status in elderly patients with knee OA.
The major findings from this study are as follows 1) ten sessions of knee acupuncture added SP6 acupoint significantly decreased the plasma ESR and hs-CRP, indicating that it could reduce the systemic inflammation in elderly patients with knee OA; 2) knee acupuncture added SP6 acupoint significantly increased knee flexion and knee extension in elderly patients with knee OA; and 3) knee acupuncture added SP6 acupoint significantly decreased pain in elderly patients with knee OA.
A low-grade systemic inflammation, as indicated by plasma ESR and hs-CRP, was found in an active OA that affected the large joint, especially knee joint (Attur et al., 2015; Robinson et al., 2016; Sanchez-Ramirez et al., 2013; Sanchez-Ramirez et al., 2014). In the present study, we found that addition of the SP6 acupoint to a traditional knee acupuncture could decrease both plasma ESR and hs-CRP levels. At the molecular levels of underlying mechanism might be due to the fact that knee acupuncture added SP6 acupoint treatment could promote the anti-inflammatory cytokines, such as IL-4, IGF, IL-10, and TGF-β, leading to modulate low-grade inflammation which occur in knee OA (Nees et al., 2019; Wojdasiewicz et al., 2014).
Previous studies from in vivo reports have demonstrated that traditional acupuncture alleviated an inflammation by reduced the levels of TNF-α, IL-1β, and IL-10 (da Silva et al., 2011; Lin et al., 2020). Furthermore, the SP6 acupoint attenuate the pain in dysmenorrhea via reducing the inflammatory cytokines (Dincer and Oskay, 2021; Liu et al., 2013). Therefore, in this study, the combination of traditional acupuncture and SP6 could show a manifest reduction of systemic low-grade inflammation in elderly patients with knee OA after treatment. Based on an inflammatory cytokines modulate pain intensity by decreasing pain threshold (de Goeij et al., 2013). In this study, we found that inflammatory cytokines and pain intensity were reduced in a similar manner. Moreover, we assumed that acupuncture could modulate the pain threshold through “gate control” theory mentioned above (Gomes and Leão, 2020; Ondrejkovicova et al., 2016).
Regarding a reduction of inflammation and pain intensity in knee OA patients treated with acupuncture added SP6, improvement in knee ROM regarded knee flexion and knee extension, were found in this study. This result could be due to an increase in systemic inflammatory cytokine can decrease the elasticity in the joint suffering from inflammation, leading to decrease joint stiffness (Choy and Panayi, 2001; Liu et al., 2022). Although this study is the first study to demonstrate the beneficial effects of acupuncture added SP6 acupoint on knee pain, knee motion, as well as systemic inflammation in elderly patients with knee OA, in order to validate the findings of this treatment in elderly patients with knee OA, a control group of traditional acupuncture is necessary to compare to the additional SP6 treatment in the further study.
CONCLUSION
Knee acupuncture added SP6 point could improve the knee motion through reducing pain and decreasing plasma inflammatory cytokines.
ACKNOWLEDGMENTS
The authors would like to thank Dr. Patchareeya Amput, PhD and Piyanuch Lonan for their technical help.
AUTHOR CONTRIBUTIONS
Conceptualization, W.K., N.S., and A.K.; Methodology, W.K., Y.T., P.J., N.S., and A.K.; Writing – Original Draft Preparation, W.K.; Writing – Review & Editing, W.K., N.S., and A.K.; Funding Acquisition, W.K. and A.K.
CONFLICT OF INTEREST
The authors declare that they hold no competing interests.
REFERENCES
Attur, M., Krasnokutsky, S., Statnikov, A., Samuels, J., Li, Z., Friese, O., Hellio Le Graverand-Gastineau, M. P., Rybak, L., Kraus, V. B., Jordan, J. M., Aliferis, C. F., and Abramson, S. B. 2015. Low-grade inflammation in symptomatic knee osteoarthritis: prognostic value of inflammatory plasma lipids and peripheral blood leukocyte biomarkers. Arthritis & Rheumatology. 67(11): 2905-2915.
Bennell, K., Hinman, R., and Wrigley, T. 2007. Chapter 13 - future directions in physical therapy for knee osteoarthritis. P.217-231 In L. Sharma & F. Berenbaum (eds.), Osteoarthritis. Philadelphia: Mosby.
Berenbaum, F. 2013. Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!). Osteoarthritis and Cartilage. 21(1): 16-21.
Brien, S. B., Bishop, F. L., Riggs, K., Stevenson, D., Freire, V., and Lewith, G. 2011. Integrated medicine in the management of chronic illness: A qualitative study. British Journal of General Practice. 61(583): e89-96.
Chew, E. S., Yeo, S. J., Haines, T., Thumboo, J., Clark, R. A., Chong, H. C., Poon, C. L. L., Seah, F. J., Tay, D. K. J., Pang, N. H., Tan, C. I. C., and Pua, Y. H. 2019. Predicting mobility limitations in patients with total knee arthroplasty in the inpatient setting. Archives of Physical Medicine and Rehabilitation. 100(11): 2106-2112.
Choy, E. H., and Panayi, G. S. 2001. Cytokine pathways and joint inflammation in rheumatoid arthritis. The New England Journal of Medicine. 344(12): 907-916.
da Silva, M. D., Guginski, G., Werner, M. F., Baggio, C. H., Marcon, R., and Santos, A. R. 2011. Involvement of interleukin-10 in the anti-inflammatory effect of sanyinjiao (SP6) acupuncture in a mouse model of peritonitis. Evidence-Based Complementary and Alternative Medicine. 2011: 217946.
de Goeij, M., van Eijk, L. T., Vanelderen, P., Wilder-Smith, O. H., Vissers, K. C., van der Hoeven, J. G., Kox, M., Scheffer, G. J., and Pickkers, P. 2013. Systemic inflammation decreases pain threshold in humans in vivo. PLoS One. 8(12): e84159.
Dincer, Y. and Oskay, U. 2021. The Effect of Acupressure Applied to Sanyinjiao (SP6) on Primary Dysmenorrhea. Alternative Therapies in Health and Medicine. 29(1): 16-22.
Feng, J. E., Novikov, D., Anoushiravani, A. A., and Schwarzkopf, R. 2018. Total knee arthroplasty: improving outcomes with a multidisciplinary approach. Journal of Multidisciplinary Healthcare. 11: 63-73.
Goggins, J., Baker, K., and Felson, D. 2005. What WOMAC pain score should make a patient eligible for a trial in knee osteoarthritis? Journal of Rheumatology. 32(3): 540-542.
Gomes, L. R., and Leão, P. 2020. Recent approaches on signal transduction and transmission in acupuncture: A biophysical overview for medical sciences. Journal of Acupuncture and Meridian Studies. 13(1): 1-11.
Gupta, S., Hawker, G. A., Laporte, A., Croxford, R., and Coyte, P. C. 2005. The economic burden of disabling hip and knee osteoarthritis (OA) from the perspective of individuals living with this condition. Rheumatology (Oxford). 44(12): 1531-1537.
Hsu, H. and Siwiec, R. M. 2023. Knee Osteoarthritis. In StatPearls. https://www.ncbi.nlm.nih.gov/pubmed/29939661
Jensen, M. P., Karoly, P., and Braver, S. 1986. The measurement of clinical pain intensity: A comparison of six methods. Pain, 27(1): 117-126.
Karsdal, M. A., Michaelis, M., Ladel, C., Siebuhr, A. S., Bihlet, A. R., Andersen, J. R., Guehring, H., Christiansen, C., Bay-Jensen, A. C., and Kraus, V. B. 2016. Disease-modifying treatments for osteoarthritis (DMOADs) of the knee and hip: Lessons learned from failures and opportunities for the future. Osteoarthritis and Cartilage. 24(12): 2013-2021.
Kiadaliri, A. A., Gerhardsson de Verdier, M., Turkiewicz, A., Lohmander, L. S., and Englund, M. 2017. Socioeconomic inequalities in knee pain, knee osteoarthritis, and health-related quality of life: A population-based cohort study in southern Sweden. Scandinavian Journal of Rheumatology. 46(2): 143-151.
Korostyshevskiy, V. 2020. Possible improvements of acupuncture for knee-pain treatment outcomes through local point palpation. Acupuncture in Medicine. 32(5): 320-324.
Kuptniratsaikul, V. and Rattanachaiyanont, M. 2007. Validation of a modified Thai version of the Western Ontario and McMaster (WOMAC) osteoarthritis index for knee osteoarthritis. Clinical Rheumatology. 26(10): 1641-1645.
Lee, J. Y., Han, K., Park, Y. G., and Park, S. H. 2021. Effects of education, income, and occupation on prevalence and symptoms of knee osteoarthritis. Scientific Reports. 11(1): 13983.
Leifer, V. P., Katz, J. N., and Losina, E. 2022. The burden of OA-health services and economics. Osteoarthritis and Cartilage. 30(1): 10-16.
Li, B., and Chen, D. 2019. Degenerative musculoskeletal diseases: Pathology and treatments. Journal of Orthopaedic Translation. 17: 1-2.
Lin, W., Jia, D., Fu, C., Zheng, Y., and Lin, Z. 2020. Electro-acupuncture on ST36 and SP6 acupoints ameliorates lung injury via sciatic nerve in a rat model of limb ischemia-reperfusion. Journal of Inflammation Research. 13: 465-470.
Liu, S., Deng, Z., Chen, K., Jian, S., Zhou, F., Yang, Y., Fu, Z., Xie, H., Xiong, J., and Zhu, W. 2022. Cartilage tissue engineering: From proinflammatory and anti‑inflammatory cytokines to osteoarthritis treatments (Review). Molecular Medicine Reports. 25(3): 99.
Liu, Y. Q., Ma, L. X., Xing, J. M., Cao, H. J., Wang, Y. X., Tang, L., Li, M., Wang, Y., Liang, Y., Pu, L. et al. 2013. Does Traditional Chinese Medicine pattern affect acupoint specific effect? Analysis of data from a multicenter, randomized, controlled trial for primary dysmenorrhea. Journal of Alternative and Complementary Medicine. 19(1): 43-49.
Minetto, M. A., Giannini, A., McConnell, R., Busso, C., Torre, G., and Massazza, G. 2020. Common musculoskeletal disorders in the elderly: The star triad. Journal of Clinical Medicine. 9(4): 1216.
Nees, T. A., Rosshirt, N., Zhang, J. A., Reiner, T., Sorbi, R., Tripel, E., Walker, T., Schiltenwolf, M., Hagmann, S., and Moradi, B. 2019. Synovial cytokines significantly correlate with osteoarthritis-related knee pain and disability: Inflammatory mediators of potential clinical relevance. Journal of Clinical Medicine. 8(9): 1343.
Ondrejkovicova, A., Petrovics, G., Svitkova, K., Bajtekova, B., and Bangha, O. 2016. Why acupuncture in pain treatment? Neuroendocrinology Letters. 37(3): 163-168.
Paul, S., Daniel, A., Maarten de, W., Tanja, A. S., Farideh, A., Diane, L., Josef, S. S., and David, T. F. 2023. American College of Rheumatology/EULAR remission criteria for rheumatoid arthritis: 2022 revision. Annals of the Rheumatic Diseases. 82(1): 74.
Peat, G., Thomas, E., Duncan, R., Wood, L., Hay, E., and Croft, P. 2006. Clinical classification criteria for knee osteoarthritis: performance in the general population and primary care. Annals of the Rheumatic Diseases. 65(10): 1363-1367.
Phutrakool, P. and Pongpirul, K. 2022. Acceptance and use of complementary and alternative medicine among medical specialists: a 15-year systematic review and data synthesis. Systematic Reviews. 11(1): 10.
Rao, J. K., Mihaliak, K., Kroenke, K., Bradley, J., Tierney, W. M., and Weinberger, M. 1999. Use of complementary therapies for arthritis among patients of rheumatologists. Annals of Internal Medicine. 131(6): 409-416.
Robinson, W. H., Lepus, C. M., Wang, Q., Raghu, H., Mao, R., Lindstrom, T. M., and Sokolove, J. 2016. Low-grade inflammation as a key mediator of the pathogenesis of osteoarthritis. Nature reviews. Rheumatology. 12(10): 580-592.
Rudnicka, E., Napierala, P., Podfigurna, A., Meczekalski, B., Smolarczyk, R., and Grymowicz, M. 2020. The World Health Organization (WHO) approach to healthy ageing. Maturitas. 139: 6-11.
Sanchez-Ramirez, D. C., van der Leeden, M., van der Esch, M., Gerritsen, M., Roorda, L. D., Verschueren, S., van Dieen, J., Dekker, J., and Lems, W. F. 2013. Association of serum C-reactive protein and erythrocyte sedimentation rate with muscle strength in patients with knee osteoarthritis. Rheumatology (Oxford), 52(4): 727-732.
Sanchez-Ramirez, D. C., van der Leeden, M., van der Esch, M., Roorda, L. D., Verschueren, S., van Dieen, J. H., Dekker, J., and Lems, W. F. 2014. Elevated C-reactive protein is associated with lower increase in knee muscle strength in patients with knee osteoarthritis: A 2-year follow-up study in the Amsterdam Osteoarthritis (AMS-OA) cohort. Arthritis Research & Therapy. 16(3): R123.
Sangdee, C., Teekachunhatean, S., Sananpanich, K., Sugandhavesa, N., Chiewchantanakit, S., Pojchamarnwiputh, S., and Jayasvasti, S. 2002. Electroacupuncture versus diclofenac in symptomatic treatment of osteoarthritis of the knee: A randomized controlled trial. BMC Complementary and Alternative Medicine. 2: 3.
Schell, J., Scofield, R. H., Barrett, J. R., Kurien, B. T., Betts, N., Lyons, T. J., Zhao, Y. D., and Basu, A. 2017. Strawberries improve pain and inflammation in obese adults with radiographic evidence of knee osteoarthritis. Nutrients. 9(9): 949.
Seyed Hashemi, M., Namiranian, N., Tavahen, H., Dehghanpour, A., Rad, M. H., Jam-Ashkezari, S., Emtiazy, M., and Hashempur, M. H. 2021. Efficacy of pomegranate seed powder on glucose and lipid metabolism in patients with type 2 diabetes: a prospective randomized double-blind placebo-controlled clinical trial. Complementary Medicine Research. 28(3): 226-233.
Tang, L., Jia, P., Zhao, L., Kang, D., Luo, Y., Liu, J., Li, L., Zheng, H., Li, Y., Li, N., Guyatt, G., and Sun, X. 2018. Acupuncture treatment for knee osteoarthritis with sensitive points: Protocol for a multicentre randomised controlled trial. BMJ Open. 8(10): e023838.
Teixeira, J., Santos, M. J., Matos, L. C., and Machado, J. P. 2018. Evaluation of the effectiveness of acupuncture in the treatment of knee osteoarthritis: A case study. Medicines (Basel), 5(1): 18.
Wang, C. 2013. Complementary and Alternative Medicine and Osteoarthritis. Journal of Integrative Medicine. 1: 13.
Wilkins, A. N. and Phillips, E. M. 2008. Chapter 61 - Knee osteoarthritis. P. 345-353. In W. R. Frontera, J. K. Silver, & T. D. Rizzo (eds.) Essentials of physical medicine and rehabilitation (Second Edition). Philadelphia: W.B. Saunders.
Wojdasiewicz, P., Poniatowski, Ł. A., and Szukiewicz, D. 2014. The role of inflammatory and anti-inflammatory cytokines in the pathogenesis of osteoarthritis. Mediators of Inflammation. 2014: 561459.
OPEN access freely available online
Natural and Life Sciences Communications
Chiang Mai University, Thailand. https://cmuj.cmu.ac.th
Warangkhana Klajing1, Natticha Sumneang2, Yin Shen Tan1, Pongnared Jaengpromma1, and Anongporn Kobroob3, *
1 Department of Traditional Chinese Medicine, School of Public Health, University of Phayao, Phayao 56000, Thailand.
2 Department of Medical Science, School of Medicine, Walailak University, Nakhon Si Thammarat 80160, Thailand.
3 Division of Physiology, School of Medical Sciences, University of Phayao, Phayao 56000, Thailand.
Corresponding author: Anongporn Kobroob E-mail: anongporn.ko@up.ac.th
Total Article Views
Editor: Veerasak Punyapornwithaya,
Chiang Mai University, Thailand
Article history:
Received: October 6, 2022;
Revised: June 8, 2023;
Accepted: June 13, 2023;
Published online: June 29, 2023